Retrobulbar hemorrhage (RBH) is a rapidly progressive emergency condition in which blood accumulates in the retrobulbar space. Increased orbital pressure compresses and causes ischemia of the optic nerve and retinal vessels, leading to irreversible vision loss if left untreated.
It was originally described as orbital hemorrhage caused by injury to orbital vessels from a retrobulbar needle used for retrobulbar anesthesia, but in a broader sense, it includes any accumulation of blood in the orbit (orbital hematoma) due to trauma, iatrogenic injury, vascular lesions, or tumor bleeding.
Epidemiology: It is a rare condition; among 1,386 orbital trauma patients, 50 had retrobulbar hemorrhage. The incidence depends on the cause of injury. Without treatment, the blindness rate is reported to be about 48% (44–52%), but with appropriate and prompt treatment, it decreases to 0.14% 3). The incidence as a complication of retrobulbar anesthesia is 0.1–3%, but since topical anesthesia and sub-Tenon’s anesthesia have become mainstream for cataract surgery, retrobulbar hemorrhage due to retrobulbar anesthesia is rarely observed.
QWhat is the probability of blindness from retrobulbar hemorrhage?
A
Without treatment, about 48% of patients become blind, but prompt and appropriate treatment reduces the blindness rate to 0.14%. Early diagnosis and decompression are essential to prevent blindness.
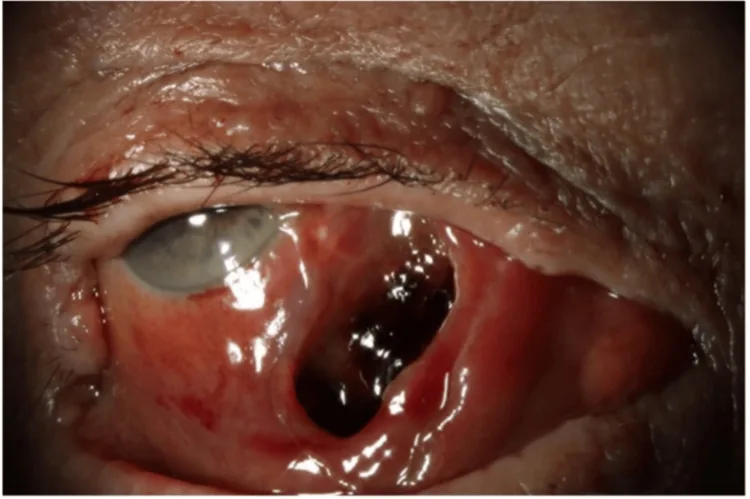
Sharif S, et al. Spontaneous Medial Rectus Haematoma: A Sight-Threatening Complication of Warfarin Toxicity. Cureus. 2025. Figure 2. PMCID: PMC11851350. License: CC BY.
Anterior segment photograph of the right eye 15 days after hematoma onset, showing extensive subconjunctival hemorrhage, a large hematoma of the medial rectus muscle, and marked deviation of the eyeball. This corresponds to the subconjunctival hemorrhage discussed in the section “2. Main symptoms and clinical findings”.
Findings confirmed by the physician during examination are as follows.
Proptosis: Forward displacement due to increased intraorbital pressure.
Elevated intraocular pressure: Intraocular pressure of 30 mmHg or higher is an indication for decompression intervention3). In severe cases, it may reach 50 mmHg or higher3).
Eyelid ecchymosis and eyelid hematoma: Observed in both traumatic and iatrogenic cases.
Subconjunctival hemorrhage: Due to blood extravasation from the retrobulbar space to the anterior region.
Ophthalmoplegia: Caused by compression of muscles or nerves due to increased intraorbital pressure or hematoma. Even with minimal proptosis and normal intraocular pressure, it may suggest progressive optic neuropathy.
Traumatic: Orbital trauma (falls, blunt trauma) is the most common cause.
Retrobulbar anesthesia: Vascular injury within the orbit due to the retrobulbar needle. Has been decreasing in recent years.
Eyelid and orbital surgery: Can occur as a postoperative complication.
Strabismus surgery: A rare complication that can occur even in the early stages of conjunctival and Tenon’s capsule incision. Inferior oblique muscle surgery carries a high risk of vortex vein injury 1).
Vascular / Coagulation Disorders
Vascular lesions: Bleeding from arteriovenous malformations, orbital varices, lymphangiomas, and hemangiomas.
Tumor-related bleeding: Hematoma formation due to hemorrhage within an orbital tumor.
Coagulation disorders: Such as idiopathic thrombocytopenic purpura (ITP) 2) and acquired hemophilia A 4).
Intracranial hemorrhage: Secondary orbital hematoma can also occur via the superior orbital fissure.
During retrobulbar anesthesia, use a sharp needle and aspirate the inner cylinder if discomfort is felt upon insertion to check for bleeding. In strabismus surgery, careful hemostasis should be performed at each step 1). Postoperative blood pressure management is also important.
QDoes taking anticoagulants increase the risk of retrobulbar hemorrhage?
A
Multiple studies have found an association between anticoagulant/antiplatelet use and retrobulbar hemorrhage 3). It is important to inform your doctor about any medications you are taking before surgery and to consider discontinuation or alternative measures as needed.
The diagnosis of retrobulbar hemorrhage is generally made clinically. Due to the urgency of treatment, diagnosis and treatment should not be delayed for imaging studies. Perform a complete ophthalmic examination (visual acuity, intraocular pressure, eye movements, pupillary response, APD assessment) promptly.
Indications for decompression intervention (if any of the following are met) 3):
Intraocular pressure ≥ 30 mmHg
Sudden vision loss
Pupillary abnormalities (loss of light reflex, abnormal dilation)
CT is useful for visualizing the orbit and is performed when associated injuries need to be ruled out or when the source of bleeding is unclear. Hematomas appear as hyperdense areas (CT value 40–80 HU) on CT; subperiosteal hematomas show a well-defined hyperdense area between the orbital bone and periosteum.
MRI can evaluate signal changes of the hematoma over time. The MRI signal of a hematoma changes as follows:
Phase
Main hemoglobin
T1 signal
T2 signal
Hyperacute (up to 1 day)
Oxy Hb
Mildly hypointense
Mildly hyperintense
Acute phase (1–3 days)
Deoxy Hb
Mildly hypointense
Hypointense
Subacute phase (3 days–1 month)
Met Hb
Hyperintense
Hyperintense
Chronic phase (1 month–)
Hemosiderin
Hypointense
Hypointense
MRA is useful for excluding arteriovenous malformations2).
Minor bleeding: If there are no signs of optic nerve compression, observation may be possible. In cases of minor bleeding, no specific treatment may be needed.
Compression hemostasis: Apply pressure with the palm over the eyelid for several minutes to achieve hemostasis and reduce intraorbital pressure.
If the hematoma is small and there are no signs of optic nerve compression: Consider observation with oral hemostatic agents.
If symptoms do not improve with compression or if criteria for decompression are met, prompt surgical intervention should be performed. The lateral canthal tendon, which forms the orbital compartment, is cut (cantholysis or canthotomy) to release intraorbital pressure.
First-Line Treatment
Lateral canthotomy and cantholysis (LC/IC): First-line treatment for orbital compartment syndrome. Can be performed under local anesthesia and achieves rapid decompression3).
Combined orbital septum incision: After temporary decompression by LC/IC, the orbital septum is incised to remove the hematoma and identify the bleeding source3).
Additional Procedures
Inferior septectomy: Added when LC/IC does not improve the condition.
Inferolateral orbitotomy: For cases requiring more extensive decompression.
Vertical split incision: An alternative procedure that can be performed even in facilities unfamiliar with eyelid anatomy.
Timing of intervention: Intervention within 2 hours of onset is recommended. However, surgery should be actively attempted even after 2 hours; recovery to corrected visual acuity of 20/20 has been reported with LC/IC plus orbital septum incision performed 7 hours and 4 hours after injury3).
If optic nerve damage is a concern, plan hematoma removal. The procedure involves skin incision according to the hematoma location → exposure and incision of the orbital septum and periosteum → hematoma aspiration with a suction cannula → irrigation with physiological saline. In cases of tumor bleeding, plan total excision of the tumor including the hematoma.
Management of Retrobulbar Hemorrhage Associated with Coagulation Abnormalities
If coagulation disorder is the cause, concurrent treatment of the underlying disease is necessary.
Idiopathic thrombocytopenic purpura: Reports include platelet transfusion + IVIG 1 g/kg × 2 days + dexamethasone 40 mg × 4 days + cryoprecipitate2).
Acquired hemophilia A: After temporary hemostasis with FEIBA administration, immunosuppressive therapy with prednisolone 60 mg + cyclophosphamide is performed4).
QWhat is lateral canthotomy for retrobulbar hemorrhage?
A
It is an emergency procedure in which the lateral canthus (outer corner of the eye) is incised and the lateral canthal tendon is cut superiorly and inferiorly to create an opening in the anterior orbit. It can be performed under local anesthesia and aims to rapidly lower orbital pressure and restore blood flow to the optic nerve3).
QWithin how many hours of onset should treatment for retrobulbar hemorrhage be performed?
A
Intervention within 2 hours of onset is recommended. However, surgical decompression is effective even after 2 hours, and recovery to corrected visual acuity of 20/20 has been reported even 7 hours after injury 3). Regardless of the time elapsed, it is important to perform decompression as soon as possible.
The anterior boundary of the orbital compartment is the orbital septum, which attaches to the lateral canthal tendon and the lateral orbital rim. The medial, lateral, and posterior boundaries are formed by the orbital bones, resulting in a fixed volume.
When bleeding occurs, intraorbital pressure increases, shifting the eye forward. The source of bleeding is usually the infraorbital artery or its branches, and bleeding from interfascial vessels can also occur 1). A slight forward displacement of the eye is tolerated, but when the optic nerve reaches its stretching limit, optic nerve damage occurs.
Mechanisms of blindness are as follows:
Optic nerve compression/ischemia: Direct compression due to increased intraorbital pressure.
Obstruction of optic nerve venous return: Secondary ischemia due to venous stasis.
In cases of arterial injury, a sharp increase in intraorbital pressure compresses the eye, causing optic nerve damage and retinal artery occlusion due to high intraocular pressure. Venous bleeding follows a relatively gradual course, so if the amount is small, it may be naturally absorbed with observation alone. Even in the presence of orbital fracture, persistent bleeding can increase intraocular pressure3).
The MRI signal of a hematoma changes over time depending on the oxidation and hemolysis of hemoglobin; for details, refer to the MRI signal change table in the “Diagnosis and Examination Methods” section.
7. Latest Research and Future Prospects (Investigational Reports)
Ochi et al. (2025) performed a two-stage surgery involving lateral canthotomy/cantholysis followed by orbital septum incision for two cases of traumatic retrobulbar hemorrhage 3). Case 1 (92-year-old male, on antiplatelet medication, surgery 7 hours after injury) had intraocular pressure of 55 mmHg and light perception only, which recovered to 14 mmHg and corrected visual acuity of 20/20 the next day. Case 2 (72-year-old female, surgery 4 hours after injury) had intraocular pressure of 52 mmHg and counting fingers, which recovered to 14 mmHg and corrected visual acuity of 20/20 the next day. This report suggests that favorable outcomes may be possible even beyond the conventional recommendation of decompression within 2 hours of onset.
Omar et al. (2024) reported a case of spontaneous retrobulbar hemorrhage in an 80-year-old woman with idiopathic thrombocytopenic purpura (platelet count 35,000/mm³) 2). MRI revealed a hematoma measuring 2.7 × 1.6 × 2.1 cm. Medical treatment with IVIG, cryoprecipitate, and dexamethasone increased platelet count to 126,000/mm³ and improved vision. Previously, only three cases of idiopathic thrombocytopenic purpura-associated orbital hemorrhage had been reported, all with severe anemia, but this case demonstrates that it can occur even with mild anemia (Hb 10.2 g/dL).
Gawęcki et al. (2024) reported a rare case of retrobulbar hemorrhage occurring during the early stage of conjunctival and Tenon’s capsule incision in strabismus surgery in a 5-year-old boy 1). The hemorrhage was managed with intravenous mannitol 100 mL, and orbital decompression was not required. The hematoma resolved within 24 hours postoperatively. No coagulation abnormalities were found, and postoperative OCT showed no RNFL asymmetry or optic neuropathy. The report emphasizes the importance of careful hemostasis at each surgical step.
Jayasundara et al. (2021) reported a case of spontaneous retrobulbar hemorrhage due to acquired hemophilia A (aPTT 127 seconds) in a 64-year-old man 4). Hemostasis was temporarily achieved with FEIBA, but it took about 6 weeks for aPTT to normalize with immunosuppression using prednisolone 60 mg and cyclophosphamide. Ultimately, the eye became gangrenous and spontaneously dislocated, a rare outcome. This case highlights the need to consider the possibility of factor VIII autoantibodies in non-traumatic retrobulbar hemorrhage.
Gawęcki M, Kiciński K.. Retrobulbar hemorrhage during strabismus surgery. Am J Ophthalmol Case Rep. 2024;33:101991. doi:10.1016/j.ajoc.2024.101991. PMID:38292880; PMCID:PMC10826133.
Omar KO, Sebastian W, Anees A.. Rare Case of Idiopathic Thrombocytopenia Causing Retrobulbar Hemorrhage. J Community Hosp Intern Med Perspect. 2024;14(5):124-127. doi:10.55729/2000-9666.1379. PMID:39399187; PMCID:PMC11466339.
Ochi Y, Ono S, Ogawa R.. Emergency Lateral Canthotomy Followed by Orbital Septum Release for Traumatic Retrobulbar Hemorrhage: 2 Case Reports. Plast Reconstr Surg Glob Open. 2025;13(3):e6582. doi:10.1097/gox.0000000000006582. PMID:40040946; PMCID:PMC11875615.
Jayasundara HD, Herath LY, Kularatne KS.. Retrobulbar Hemorrhage Secondary to Acquired Hemophilia A. Cureus. 2021;13(9):e17760. doi:10.7759/cureus.17760. PMID:34659972; PMCID:PMC8494152.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.