Asteroid hyalosis (AH) is a degenerative disease of the vitreous fibers that generally occurs in elderly individuals aged 60 years or older. Asteroid bodies (AB) are deposited within the collagen fibers of the vitreous, leading to vitreous degeneration. Asteroid bodies are composed mainly of calcium-containing phospholipids and mucopolysaccharides (or calcium phosphate), appearing as yellowish-white, spherical, coarse particles floating in the vitreous. They move with eye movement but return to their original position when the eye is still.
It was first described by Alfred Hugh Benson in 1894, and later named “asteroid hyalosis” by Luxenberg and Sime. It is a distinct disease from synchysis scintillans (see Differential Diagnosis).
80% are unilateral. The prevalence is about 1-2%, and three major epidemiological studies have reported the following results.
Study
Prevalence
Notes
Beaver Dam Eye Study
1.2%
Age 43-54: 0.2% → 75-86: 2.9%. Men 1.4% vs Women 0.6%5)
Blue Mountains Eye Study
1.0%
49-55 years 0% → 75-97 years 2.1%6)
UCLA autopsy cohort (10,801 individuals)
1.96%
Pathological analysis7)
Regarding sex differences, males (1.4%) are more affected than females (0.6%), and it is more common in elderly individuals aged 60 years and older.5)
An association with diabetes has often been suggested. However, none of the Beaver Dam, Blue Mountains, or UCLA studies confirmed a significant link.5)6)7) The fact that it is predominantly unilateral also raises doubts about a connection with systemic diseases.
QAre people with diabetes more likely to develop asteroid hyalosis?
A
An association with diabetes has long been suggested. However, none of the three large-scale studies—the Beaver Dam Eye Study, the Blue Mountains Eye Study, and the UCLA autopsy cohort—confirmed a significant link.5)6)7) The predominantly unilateral nature also raises doubts about a direct causal relationship with systemic diseases.
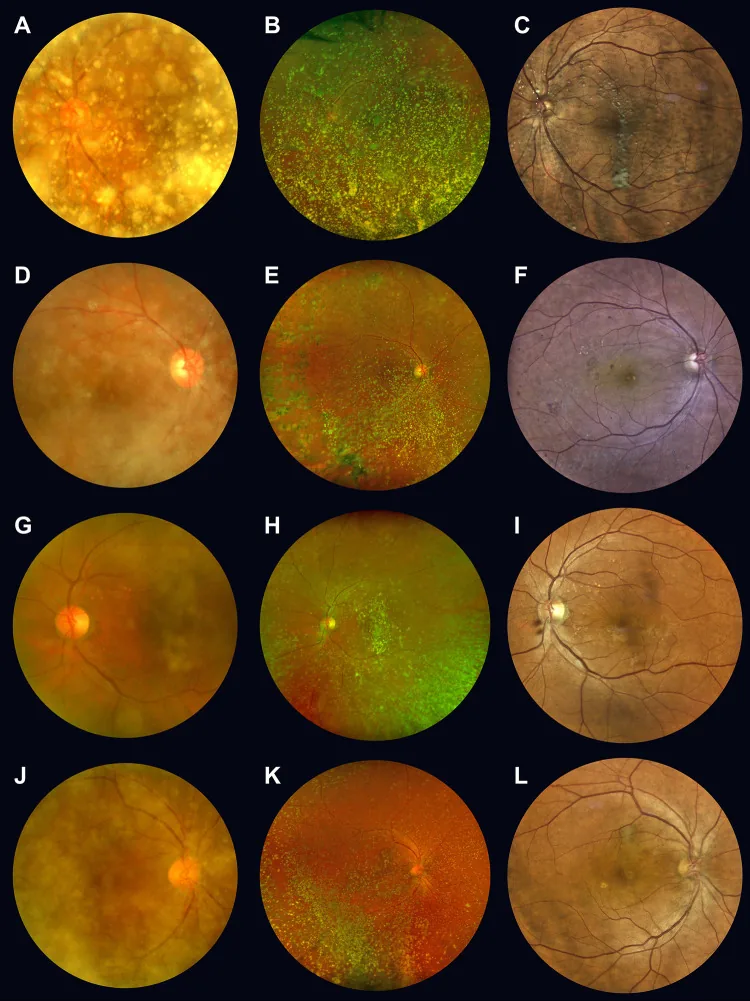
Park SH, et al. Diagnostic ability of confocal scanning ophthalmoscope for the detection of concurrent retinal disease in eyes with asteroid hyalosis. PLoS One. 2024. Figure 2. PMCID: PMC11620638. License: CC BY.
A to L are fundus photographs of the same patient with asteroid hyalosis. In A/D/J, yellow-white asteroid bodies heavily cover the optic disc and macula. This corresponds to the vitreous opacities discussed in the section “2. Main symptoms and clinical findings.”
Usually asymptomatic. Even with moderate opacities, patients often do not notice floaters, and visual acuity is good, often requiring no treatment. A characteristic feature is that even with severe opacities, visual acuity is preserved, and even advanced asteroid hyalosis that makes fundus examination difficult often does not require treatment.
Rarely, acute vision loss occurs triggered by posterior vitreous detachment (PVD). The mechanism is that asteroid bodies concentrate in the anterior vitreous, increasing the density of opacities near the nodal point of the eye and blocking the visual axis. 3)
In a case series of 6 eyes by Marlow et al., all cases presented with acute or subacute vision loss. The mean preoperative best-corrected visual acuity (BCVA) was 20/150 (range 20/25 to 20/2500), and the mean decrease associated with progression of posterior vitreous detachment was 0.70 logMAR. 3)
Observation of the anterior vitreous with a slit lamp microscope is essential. Have the patient move their eyes and observe the movement of the vitreous. With a slit lamp microscope, yellowish-white, spherical, coarse particles floating in the vitreous are observed.
They exhibit mobility with eye movement, but return to their original position when at rest. This is because the vitreous is not liquefied, and the asteroid bodies remain attached to the vitreous fibers and follow the movement. Asteroid bodies are large particles and are easily distinguished from white blood cells.
Vitreous liquefaction is often absent, and many cases do not develop posterior vitreous detachment. There is a characteristic that adhesion to the retina is strong, making posterior vitreous detachment less likely. When posterior vitreous detachment occurs in asteroid hyalosis eyes, it is often accompanied by vitreoschisis due to abnormal vitreoretinal adhesion. 3)
Note on severe opacity: In cases of proliferative diabetic retinopathy, retinal photocoagulation is often difficult, and vitreous surgery may also be challenging.
QCan vision suddenly become difficult to see?
A
Usually asymptomatic, but acute vision loss can occur triggered by posterior vitreous detachment (PVD). This is because asteroid bodies concentrate in the anterior vitreous and block the visual axis. 3) In the report by Marlow et al., even in the group of cases with mean preoperative visual acuity decreased to 20/150, all cases recovered to baseline visual acuity within 3 months after PPV. 3)
Aging is the greatest risk factor. It is generally seen in elderly people aged 60 years and older. Associations with the following factors have also been reported.
Aging: Prevalence increases with age, notably increasing after age 75. 5)
Male sex: Prevalence is higher in males (1.4%) compared to females (0.6%). 5)
Hypertension, hypercholesterolemia, elevated serum calcium: Some reports suggest an association. 5)
Diabetes: Often seen in diabetic patients and the elderly, but the causal relationship is unclear. None of the three major epidemiological studies showed a significant difference5)6)7)
Observation of the anterior vitreous using a slit-lamp microscope is essential. Diagnosis can be made by having the patient move their eyes and observing the movement of the vitreous. The key to diagnosis is the presence of characteristic yellowish-white spherical opacities in the vitreous that move with eye movement and return to their original position when at rest. These are large particles derived from calcium crystals, making diagnosis relatively easy.
High-intensity focus without posterior echo defect
When fundus is not visible
OCT: 830 nm wavelength is less affected by asteroid bodies and is useful for evaluating the vitreoretinal interface. However, dense AH may absorb and reflect light, causing shadowing.
Usually, patients are unaware of floaters and have good vision, so treatment is often unnecessary. Even with severe opacities, vision is often preserved, and surgery is rarely indicated.
The treatment flow is as follows:
No symptoms, good vision → Observation (no treatment needed)
Severe opacity causing visual impairment → Consider vitrectomy
Cases with diabetic retinopathy → If asteroid bodies interfere with photocoagulation, perform photocoagulation after vitrectomy (opacity removal)
Planned cataract surgery → Check accuracy of refractive and axial length measurements preoperatively (be aware of errors)
Surgery is indicated when visual impairment occurs. If opacities are severe and cause visual impairment, vitrectomy is performed. In cases of acute vision loss due to posterior vitreous detachment, vitrectomy can restore vision curatively. 3)
Indications and Outcomes of Vitrectomy
Indications: When opacities are severe and cause visual impairment
Surgical technique: 23G or 25G transconjunctival vitrectomy3)
Visual recovery course: At 1 month postoperatively, 2 eyes recovered baseline vision; at 3 months, all eyes recovered3)
Final best-corrected visual acuity: Mean 20/35 (range 20/20 to 20/200)3)
Postoperative complications: None reported3)
Precautions during cataract surgery
Axial length/refractive measurement errors: Measurement errors in refractive values or axial length may occur, requiring caution during cataract surgery
Anterior chamber migration (intraoperative): A rare complication where asteroid bodies migrate into the anterior chamber during I/A manipulation1)
Anterior chamber migration (late postoperative): Can also occur due to aqueous humor reflux, such as in malignant glaucoma2)
In vitrectomy for AH eyes, vitreous liquefaction is less likely to occur and the adhesion between the posterior vitreous cortex and retina is pathologically strong, requiring careful manipulation. When complicated by proliferative diabetic retinopathy, retinal photocoagulation becomes difficult, and the difficulty of vitrectomy also increases.
Saeed et al. reported a case of a 70-year-old man in whom a yellowish-white spherical body migrated into the anterior chamber during cataract surgery (during I/A manipulation). No capsular rupture or zonular damage. It was aspirated and removed with I/A, and an IOL was inserted into the capsule. Postoperative visual acuity was 20/20 and remained good after 4 years.1)
Desai et al. reported a 70-year-old man who presented with yellow crystalline deposits in the anterior chamber, IOP 35 mmHg, and shallow anterior chamber 2 months after cataract surgery. They diagnosed anterior chamber migration of AH due to malignant glaucoma. Anterior chamber irrigation + vitreous biopsy + irido-zonulo-vitrectomy was performed, and the next day IOP improved to 17 mmHg. This demonstrated that AH anterior chamber migration can occur due to aqueous humor reflux even without posterior capsule defect or zonular weakness.2)
QWill it not recur after surgery?
A
Since vitrectomy removes the asteroid bodies along with the vitreous, no postoperative recurrence has been reported. In all 6 eyes in Marlow et al., baseline visual acuity recovered within 3 months postoperatively, and no complications were observed.3)
Asteroid bodies are thought to deposit within the collagen fibers of the vitreous, leading to vitreous degeneration. The main components are calcium-containing phospholipids, mucopolysaccharides (or calcium phosphate). Deposition on vitreous collagen fibers is the basic pathology, and although an association with diabetes has been suggested, large-scale epidemiological studies have refuted this. 5)6)7)
Electron spectroscopic imaging shows uniform distribution of Ca, P, and O, indicating structural and elemental similarity to hydroxyapatite. Immunofluorescence microscopy detects chondroitin-6-sulfate around asteroid bodies, and lectin-gold labeling confirms that hyaluronic acid-specific carbohydrates form part of the internal matrix. Proteoglycans and glycosaminoglycan (GAG) side chains are thought to be involved in regulating the biomineralization process. 8)
Relationship between AH and posterior vitreous detachment (PVD)
The vitreous is often not liquefied, and adhesion to the retina is strong, making posterior vitreous detachment less likely. However, once posterior vitreous detachment occurs, abnormal vitreoretinal adhesion tends to result in anomalous PVD with vitreoschisis. 3)
Marlow et al. confirmed partial posterior vitreous detachment (vitreoschisis) in 3 of 6 eyes. When vitreoschisis occurs, the anterior vitreous containing asteroid bodies concentrates near the nodal point of the eye, leading to visual impairment. 3)
In the pathological analysis by Topilow et al., 81% of AH eyes had microscopically normal vitreous gel, and 19% showed moderate liquefaction (syneresis). 1)
Intraoperative AH anterior chamber migration is thought to result from vitreous liquefaction (syneresis) and forward movement of asteroid bodies through microscopic zonular gaps. 1) Another mechanism for late postoperative forward migration is aqueous humor reflux due to malignant glaucoma. 2) It is important that AH anterior chamber migration can occur even without posterior capsule defects or zonular weakness. 1)2)
7. Latest research and future perspectives (reports at research stage)
Swept-source OCT (SS-OCT, central wavelength 1050 nm) has greater penetration depth than conventional SD-OCT (840 nm) and may contribute to detailed evaluation of the vitreous, choroid, and retina in eyes with asteroid hyalosis. It is expected to be less affected by light scattering from asteroid bodies, and its application to monitoring of diabetic retinopathy and macular diseases complicated by asteroid hyalosis is being investigated.
Swept-source biometry (e.g., IOLMaster 700) uses a 1050 nm wavelength, which may improve the accuracy of axial length measurement in eyes with asteroid hyalosis. In conventional optical biometry, interference from asteroid bodies can cause axial length errors, but longer wavelengths and improved signal processing are expected to increase measurement success rates. It is attracting attention as a preoperative examination option for asteroid hyalosis patients scheduled for cataract surgery.
Vitreolytic enzymes such as ocriplasmin (microplasmin) are approved for vitreomacular traction syndrome and macular holes, but their indication for asteroid hyalosis has not been established. Since the vitreous is non-liquefied in asteroid hyalosis, the efficacy and safety of pharmacologic approaches are currently unknown, and further research is needed.
Saeed O, Bloom J, Mihok B. Asteroid hyalosis migration into the anterior chamber during cataract surgery. Case Rep Ophthalmol. 2023;14:245-249.
Desai A, Kaza H, Takkar B, Choudhari N. Anterior migration of asteroid hyalosis due to aqueous misdirection: asteroids in the wrong orbit. BMJ Case Rep. 2021;14:e246441.
Marlow E, Hassan T, Faia L, Drenser K, Garretson B. Vitrectomy for symptomatic asteroid hyalosis. J VitreoRetinal Dis. 2021;5:420-424.