Avacincaptad pegol (ACP) is a pegylated RNA aptamer that binds to complement C5. Its brand name is IZERVAY. Developed by Astellas Pharma, it is provided as an intravitreal injection solution. In August 2023, the U.S. FDA approved it as a treatment for geographic atrophy (GA) secondary to age-related macular degeneration1). It is the second approved drug for GA, following the complement C3/C3b inhibitor pegcetacoplan (Syfovre) 2).
GA (geographic atrophy) is an advanced form of age-related macular degeneration that causes irreversible vision loss due to atrophy of the retinal pigment epithelium (RPE), photoreceptors, and choriocapillaris1). The global prevalence of GA is approximately 8.7%, affecting about 5 million people worldwide (1–1.6 million in the U.S.) 1). It is a leading cause of central vision loss in people over 55, with a prevalence of 3.5% at age 75 and about 22% at age 90 and older 1). Approximately 20% of legal blindness cases in the U.S. and about 26% in the U.K. are attributed to GA 3). In Japan, it occurs in men and women over 50 (male:female ≈ 3:1), starting with metamorphopsia and central scotoma, and progressing to corrected visual acuity below 0.1.
QWhat kind of drug is avacincaptad pegol?
A
It is a pegylated RNA aptamer that inhibits complement C5. Approved by the FDA in 2023 as a treatment for geographic atrophy, it slows the enlargement of GA lesions, but has not been shown to restore atrophied tissue or improve vision at this time. See the [Standard Treatment] section (#5-standard-treatment) for details.
Irreversible central vision loss: When the lesion reaches the fovea, irreversible vision loss occurs1).
GA causes slower vision loss than neovascular age-related macular degeneration, but its long-term impact on visual function is significant2). Over 2 years, approximately 75% of affected eyes lose 5 letters, about 50% lose 10 letters (3 lines), and about 25% lose 15 letters (6 lines)3). GA progression negatively affects quality of life (both vision-related and health-related), and is associated with difficulties in independent living and mental health3). Increased depression and anxiety have also been reported4).
QHow quickly does vision decline in geographic atrophy?
A
Over 2 years, approximately 75% of eyes lose 5 letters (1 line), about 50% lose 10 letters (3 lines), and about 25% lose 15 letters (6 lines) of vision3). A single lesion involving the fovea carries a high risk of vision loss, while multiple lesions have faster enlargement but relatively slower impact on vision4).
Atrophic area: Well-demarcated hypopigmented area with scalloped borders.
Surrounding findings: Drusen and pigment changes are observed around the lesion.
Lesion phenotype: Well-defined zone of atrophy of the RPE and/or choriocapillaris2).
FAF and OCT
Fundus autofluorescence (FAF): Dark hypoautofluorescence due to lack of lipofuscin. The surrounding hyperautofluorescence pattern predicts the rate of GA enlargement.
OCT (outer retina): Loss of outer nuclear layer, ellipsoid zone (EZ), and interdigitation zone; loss of RPE; increased choroidal hypertransmission. EZ integrity is useful for predicting visual prognosis4).
Subfoveal/unifocal lesions: Slow enlargement, but significant decrease in best-corrected visual acuity due to foveal involvement4).
Multifocal lesions: Rapid enlargement, but relatively slow decline in best-corrected visual acuity4).
GA growth rate: Faster growth rate is associated with faster decline in best-corrected visual acuity3).
Microperimetry: Residual retinal function may exist even within the GA area on FAF4).
Genetic predisposition: Polymorphisms in complement-related genes (CFH, CFB, C3) and ARMS2 are associated with susceptibility to age-related macular degeneration and GA1)2).
Diet and physical inactivity: Poor diet and lack of exercise increase risk1).
Pathological background: Drusen accumulation induces photoreceptor and RPE degeneration, progressing to atrophy 1). Abnormal activation of the complement system plays a key role in the onset and progression of GA 1)3). Precursor lesions of GA include retinal pigment epithelium abnormalities (pigment mottling, hyperpigmentation, hypopigmentation) and soft drusen.
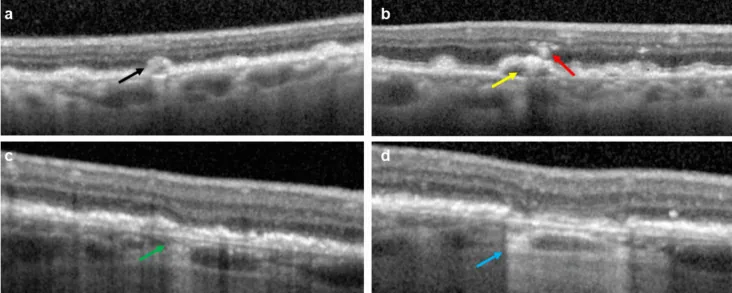
Giulia Corradetti; Ayesha Karamat; Sowmya Srinivas; Sophiana Lindenberg; Swetha B Velaga; Federico Corvi. Progression to complete retinal pigment epithelium and outer retinal atrophy (cRORA): post hoc analysis of the GATHER1 trial. Graefes Arch Clin Exp Ophthalmol. 2025 Nov 14; 263(3):669-677 Figure 1. PMCID: PMC11953152. License: CC BY.
Representative images of OCT features of interest. (a) Larger drusen ≥ 40 µm in height (black arrow), (b) drusen with hyporeflective core (yellow arrow) and intraretinal hyperreflective foci (red arrow), (c) incomplete retinal pigment epithelium and outer retinal atrophy (iRORA, green arrow), and (d) conversion to complete retinal pigment epithelium and outer retinal atrophy at a follow-up visit (cRORA, blue arrow)
A combination of multimodal imaging is recommended for the diagnosis of GA 2).
The characteristics of each examination are shown below.
Fundus autofluorescence (FAF): Standard test for GA measurement. Delineates GA lesions as areas of hypoautofluorescence. Surrounding hyperautofluorescence patterns predict progression rate.
OCT: Visualizes outer retinal loss, RPE loss, and increased choroidal transmission. Integrity of the ellipsoid zone (EZ) is useful for predicting visual prognosis4).
Microperimetry: Evaluates retinal sensitivity in detail. Can detect residual function even in GA areas, and integration with OCT biomarkers via machine learning for visual function prediction is being explored4).
Differential diagnosis: Requires differentiation from neovascular age-related macular degeneration (exudative type) and other causes of RPE atrophic changes.
In the 12-month results of GATHER2 by Khanani et al. (2023), the ACP group (n=271) showed a significant suppression of GA growth rate compared to the sham group (n=269): 0.336 vs. 0.392 mm/year (difference 0.056 mm/year; 95%CI 0.016–0.096; p=0.006)6).
The 24-month data from GATHER2 showed a 14% reduction in the monthly dosing group and a 19% reduction in the group that switched from monthly to every-other-month dosing after 12 months2).
No significant improvement in best-corrected visual acuity was shown in either GATHER1 or GATHER21)2). However, a post-hoc analysis suggested that loss of 15 or more letters in best-corrected visual acuity occurred in 4.0% of the ACP group vs. 7.6% in the sham group, and the risk of sustained 15-letter loss was reduced by 56% (HR 0.44; 95%CI 0.21–0.92)1)5).
The complement C3/C3b inhibitor pegcetacoplan (Syfovre) showed a 21% reduction in GA enlargement at 12 months with monthly dosing in the OAKS/DERBY Phase 3 trials (OAKS trial)2).
No cases of endophthalmitis or ischemic optic neuropathy were reported over 12 months1). Elevated intraocular pressure was mainly transient and related to the injection procedure1).
Risk of macular neovascularization conversion: In GATHER1, the ACP 2mg group had 9.0% vs sham 2.7%; in GATHER2, ACP 2mg group had 6.7% vs sham 4.1%1). If macular neovascularization (choroidal neovascularization) develops, treatment with anti-VEGF therapy is necessary2).
Contraindications: Patients with ocular or periocular infections, or active intraocular inflammation.
QDoes avacincaptad pegol improve vision?
A
The GATHER trials did not show significant improvement in best-corrected visual acuity1)2). However, a post-hoc analysis suggested a 56% reduction in the risk of sustained vision loss of 15 letters or more (HR 0.44), indicating a potential contribution to long-term vision maintenance5).
QWhat is the risk of choroidal neovascularization?
A
In the integrated data from the GATHER study, macular neovascularization conversion was observed in 7% of the treatment group and 4% of the sham group 2). When macular neovascularization occurs, it is managed with anti-VEGF therapy. Regular OCT monitoring is essential.
The complement system consists of three pathways: the classical pathway, the lectin pathway, and the alternative pathway 1). All three pathways converge at the cleavage of C3 by C3 convertase (C3 → C3a + C3b) 1). Subsequently, C5 convertase cleaves C5 into C5a (anaphylatoxin) and C5b 1).
C5a: An anaphylatoxin that causes recruitment and activation of inflammatory cells 1).
C5b → MAC (membrane attack complex, C5b-9): C5b-9 inserts into the cell membrane, inducing membrane lysis and cell death 1). Excessive accumulation of MAC causes lysosomal overload in RPE cells and stimulates the release of pro-inflammatory factors 1).
With aging, the expression of complement system-related genes is upregulated 1). Genetic polymorphisms in CFH, CFB, C3, and ARMS2 are associated with GA susceptibility 1)2).
ACP is a chemically synthesized single-stranded oligonucleotide, and pegylation provides biological stability and delayed clearance 1).
It binds with high affinity to C5 and inhibits its cleavage into C5a and C5b 1).
Theoretical advantage of C5 inhibition: It preserves C3a (which has anti-inflammatory and host defense functions) upstream of C5 while blocking inflammasome recruitment and MAC formation 1). In contrast to C3 inhibitors, which may impair host defense functions from upstream, C5 inhibition is considered a more selective target 1).
QWhy is complement C5 considered a therapeutic target for GA?
A
C5 cleavage products, C5a and MAC, are thought to promote GA progression through inflammatory damage to the RPE1). Inhibiting C5 prevents MAC formation and C5a generation while preserving the anti-inflammatory and host defense functions of upstream C3a. Since C3 inhibition raises concerns about increased infection risk, C5 is considered a safer target 1).
7. Latest Research and Future Perspectives (Investigational Reports)
In the 24-month data from GATHER2, GA area enlargement was suppressed by 14% in the monthly dosing group and by 19% in the group that switched to every-other-month dosing after 12 months 2). This suggests that switching to every-other-month dosing may not reduce the GA suppression rate, and optimization of dosing intervals remains a future challenge.
A post-hoc analysis suggested a 56% reduction in the risk of sustained vision loss of 15 letters or more (HR 0.44), but this is a post-hoc exploratory analysis and not a definitive conclusion 1)5). Prospective trials with visual endpoints as primary outcomes are needed for verification.
The utility of EZ (ellipsoid zone) integrity as a biomarker is being explored 1). Research on predicting visual function from OCT biomarkers using machine learning is also progressing 4). The importance of early detection and early treatment intervention for GA is emphasized 1), and these biomarkers are expected to be established as prognostic tools.
Elucidation of Mechanisms of Macular Neovascularization Conversion
Elucidating the mechanism by which complement inhibition increases the risk of developing macular neovascularization (choroidal neovascularization) remains an important unresolved issue 1). There is a hypothesis that the complement system is also involved in the suppression of angiogenesis, and understanding this balance is thought to influence future drug design.
Danzig CJ, Khanani AM, Loewenstein A. C5 inhibitor avacincaptad pegol treatment for geographic atrophy: a comprehensive review. Immunotherapy. 2024;16(12):779-790.
American Academy of Ophthalmology Retina/Vitreous Panel. Age-Related Macular Degeneration Preferred Practice Pattern. Ophthalmology. 2025;132:P1-P102.
Anegondi N, Steffen V, Sadda SR, et al. Visual loss in geographic atrophy: learnings from the lampalizumab trials. Ophthalmology. 2025;132:420-430.
Dinah C, et al. Functional endpoints in geographic atrophy clinical trials: a comprehensive review. Prog Retin Eye Res. 2026;110:101421.
Danzig CJ, Khanani AM, Kaiser PK, et al. Vision loss reduction with avacincaptad pegol for geographic atrophy: a 12-month post hoc analysis of the GATHER1 and GATHER2 trials. Ophthalmol Retina. 2024.
Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402:1449-1458.
Jaffe GJ, Westby K, Csaky KG, et al. C5 inhibitor avacincaptad pegol for geographic atrophy due to age-related macular degeneration. Ophthalmology. 2021;128:576-586.
Patel SS, Lally DR, Hsu J, et al. Avacincaptad pegol for geographic atrophy secondary to age-related macular degeneration: 18-month findings from the GATHER1 trial. Eye. 2023;37:3551-3557.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.