In blunt ocular trauma, compression and rebound stretching occur at the posterior pole, along with traction on the retina by the vitreous base. This causes tears in equatorial and peripheral retinal degenerations, as well as posterior pole tears near the vascular arcades, retinal dialysis, and ciliary epithelial tears; these are collectively called traumatic retinal tears.
Traumatic retinal tears are classified into the following three types based on location and mechanism.
Retinal dialysis: The retina detaches from the vitreous base at the far periphery (ora serrata). Common in young people.
Ciliary epithelial tear: The ciliary epithelium tears. Scleral depression is needed for diagnosis.
Retinal dialysis differs from flap tears in that it is a full-thickness split (disinsertion) and the retinal flap does not flip. The anterior edge of the retina remains attached to the ora serrata, while the posterior edge often bends toward the vitreous side.
Ora serrata tears (retinal dialysis) are common in young people. They occur particularly after blunt ocular trauma from sports injuries (boxing, soccer, baseball, etc.), traffic accidents, and assault.
In young people, vitreous liquefaction is not advanced, so the adhesion between the vitreous and retina is stronger than in adults. Therefore, traction during blunt trauma directly affects the ora serrata, making detachment more likely. On the other hand, because vitreous liquefaction is minimal, the inflow of subretinal fluid is slow, leading to a shallow retinal detachment. This “slow progression” can result in an interval of several weeks to months between injury and diagnosis.
QHow is an ora serrata tear different from a common retinal tear?
A
Common retinal tears (degenerative tears or horseshoe tears associated with posterior vitreous detachment) are more common in middle-aged and elderly people and tend to occur in the equatorial to posterior pole of the retina. In contrast, ora serrata tears are traumatic and involve detachment of the far periphery (ora serrata) from the vitreous base. The main features are that they are full-thickness gaps rather than flap tears, they occur in young people, and they progress slowly as shallow retinal detachments. They are easily missed with routine indirect ophthalmoscopy, and examination of the far periphery using a scleral depressor is necessary for diagnosis.
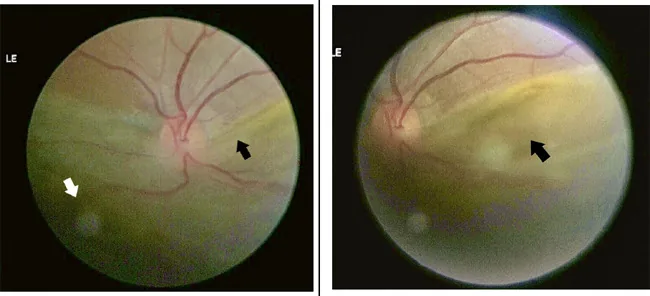
Color photograph of the posterior segment shows extensive elevation of the inferior retina and a detached edge at the ora serrata (arrow). This corresponds to the ora serrata tear discussed in the section “Main symptoms and clinical findings.”
Asymptomatic (early stage): If the ora serrata tear is small and retinal detachment has not occurred, there may be no subjective symptoms for some time after injury.
Visual field defect: If the tear is large and progresses to retinal detachment, the visual field corresponding to the tear site is lost. Since the tear is often in the inferior area, the superior visual field is often affected.
Decreased visual acuity: Occurs when retinal detachment involves the macula. In the shallow detachment stage, visual acuity may be relatively preserved.
Detachment at the ora serrata: An arcuate or semicircular full-thickness gap is seen in the far periphery. The anterior edge (ora serrata side) remains attached, and the posterior edge is folded.
Shallow peripheral retinal detachment: In young individuals with minimal vitreous liquefaction, subretinal fluid accumulates slowly and the detachment height is low.
Vitreous hemorrhage: Caused by disruption of retinal blood vessels due to trauma. It reduces the clarity of the fundus view.
Angle recession: A condition where the iris root is displaced posteriorly due to blunt trauma. It is a risk factor for traumatic glaucoma.
Schwartz syndrome refers to elevated intraocular pressure associated with a retinal dialysis at the ora serrata. The mechanism is that photoreceptor outer segments escape through the retinal break into the anterior chamber, obstructing the trabecular meshwork (the eye’s drainage structure). Medical treatment with intraocular pressure-lowering medications alone is often insufficient, and definitive treatment of the retinal break is required.
QIs examination necessary even if there are no symptoms after injury?
A
Yes, it is necessary. Retinal dialysis is often asymptomatic in the early stages and tends to be discovered late as a slowly progressive shallow retinal detachment. In young individuals who have sustained ocular trauma (especially blunt trauma), it is important to perform dilated fundus examination and cycloscopy to carefully observe the peripheral retina, including the far periphery, even in the absence of symptoms. Delayed detection can lead to proliferative vitreoretinopathy (PVR), making treatment difficult.
Blunt ocular trauma is the main cause. When the eyeball is compressed anteroposteriorly, the equator expands in the coronal plane, and the vitreous base strongly pulls on the ora serrata. In young individuals, the adhesion between the vitreous and retina is strong, so this traction force is directly transmitted to the far peripheral retina, causing a dialysis.
Young age: Because vitreous liquefaction is minimal and adhesion to the retina is strong, the traction force from blunt trauma concentrates on the ora serrata.
Sports injuries: Boxing (blows to the face) and ball injuries (soccer, baseball, tennis, racquetball) are particularly common.
Traffic accidents, occupational injuries, assault: Any blunt ocular trauma is a risk.
Peripheral retinal degeneration such as lattice degeneration: Pre-existing retinal weakness makes breaks and dialyses more likely.
Ora serrata tears occur in the far periphery, so they are easily missed with standard direct ophthalmoscopy or indirect ophthalmoscopy under mydriasis. Use of a cyclodialysis lens (scleral depressor) is essential for observing the far periphery.
Caution is needed because vitreous hemorrhage may hide a tear. Ciliary body mirror is useful for observing tears at the ora serrata and ciliary epithelium.
When the fundus is not visible: Use B-mode ultrasound to check for retinal detachment.
Non-traumatic rhegmatogenous retinal detachment: Common in middle-aged and older adults with myopia. No history of trauma. Often has horseshoe-shaped tears.
QWhat to do when the fundus is not visible due to vitreous hemorrhage?
A
B-mode ultrasonography is essential. Evaluate the presence of retinal detachment (continuity with the optic disc), extent of detachment, and presence of intraocular foreign bodies. If retinal detachment is confirmed on B-mode, early surgery is indicated. After the hemorrhage subsides, perform a detailed peripheral fundus examination including with a scleral depressor to confirm the location and size of the ora serrata tear.
Treatment strategy is determined by the presence of retinal detachment, type of trauma (open or closed globe), and size of the tear.
Without Retinal Detachment
Treatment: Laser photocoagulation
Laser is applied around the tear to create adhesion between the retina and retinal pigment epithelium. This prevents inflow of subretinal fluid and progression to retinal detachment.
Note: Small ora serrata tears may enlarge later as vitreous liquefaction progresses. Regular follow-up is necessary.
With Retinal Detachment (Closed Globe Injury, Good Media Clarity)
Treatment: Scleral buckling (encircling) surgery
Except for advanced giant retinal tears, scleral buckling is the basic procedure. The tear site is indented using a silicone sponge or silicone band to close the break. Cryopexy is used to fix the retina around the tear.
When accompanied by retinal detachment (open globe injury)
Treatment: Vitrectomy
The primary treatment goal is to release traction from incarcerated vitreous gel, and vitrectomy is relatively urgent. It also helps reduce the risk of endophthalmitis and remove intraocular foreign bodies.
For giant retinal tear detachment
Treatment: Vitrectomy + tamponade
Tamponade with silicone oil, SF6 gas (20–25%), or C3F8 gas (14–16%) is used to close the tear. Silicone oil is chosen when proliferative vitreoretinopathy (PVR) is present.
When Schwartz syndrome (elevated intraocular pressure associated with traumatic retinal detachment) is present, intraocular pressure should be temporarily managed with pressure-lowering medications (carbonic anhydrase inhibitors, beta-blockers), while definitive treatment of the retinal tear (photocoagulation or surgery) is necessary. Miotics (pilocarpine) do not contribute to suppressing aqueous humor production and are not first-line therapy.
QCan an ora serrata tear be treated with laser alone?
A
For an ora serrata tear without retinal detachment, laser photocoagulation is indicated. Laser is applied around the tear to create adhesion between the retina and retinal pigment epithelium, preventing fluid from flowing into the subretinal space. However, if the tear is large, located inferiorly, or if vitreous liquefaction is advanced with strong traction, there is a risk of progression to retinal detachment even after laser. If retinal detachment is present, surgery (scleral buckling or vitrectomy) is required.
When the eyeball is compressed anteroposteriorly by blunt trauma, the equator expands in the coronal direction (shortening of the anteroposterior diameter and enlargement of the equatorial diameter). This deformation causes the vitreous base to strongly pull the ora serrata (the peripheral border of the retina) inward.
In young individuals, vitreous liquefaction is not advanced. The vitreous gel remains homogeneous and adheres firmly to the retina, so traction is not evenly distributed over a wide area but concentrates at the ora serrata where adhesion is strongest. As a result, a full-thickness retinal tear occurs at the ora serrata.
If the tear is small, the inflow of subretinal fluid is slow, resulting in a shallow retinal detachment. In young individuals with minimal vitreous liquefaction, it takes time for fluid to spread under the retina, and progression is slow. This is why there is often a long interval between injury and diagnosis.
In traumatic retinal detachment, outer segments of photoreceptors may flow out from the edge of the tear along with subretinal fluid into the anterior chamber. These outer segments physically obstruct the trabecular meshwork (the drainage structure of the eye), impeding aqueous humor outflow and raising intraocular pressure. This condition is called Schwartz syndrome. Intraocular pressure improves with treatment of the retinal tear.
Proliferative vitreoretinopathy (PVR): Fibrous proliferative membranes form on the retinal surface or subretinally due to long-standing retinal detachment. Early treatment is extremely important as it becomes refractory.
The prognosis is good if retinal reattachment is achieved through early detection and treatment. If treatment can be performed before the macula detaches, good postoperative visual recovery can be expected. On the other hand, if detection is delayed and PVR develops, the surgical success rate decreases and the visual prognosis is poor.
Ghafour IM, Foulds WS, Allan D, et al. Causes of low visual acuity in children referred to eye clinics. Br J Ophthalmol. 1983;67:35-37.
Tasman W. Retinal detachment in children. Trans Am Acad Ophthalmol Otolaryngol. 1967;71:455-460.
Billington BM, Leaver PK, McLeod D. Management of retinal detachment in the Marfan syndrome. Trans Ophthalmol Soc U K. 1985;104:689-694.
Ambresin A, Wolfensberger TJ, Bovey EH. Management of giant retinal tears with vitrectomy, internal tamponade, and peripheral 360 degrees retinal photocoagulation. Retina. 2003;23:622-628. doi:10.1097/00006982-200310000-00003.
Ross WH.. Traumatic retinal dialyses. Arch Ophthalmol. 1981;99(8):1371-1374. doi:10.1001/archopht.1981.03930020245005. PMID:7259608.
Smiddy WE, Flynn HW.. Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004;137(3):525-537. doi:10.1016/j.ajo.2003.12.011. PMID:15013877.
Küchle M, Naumann GO. Direct cyclopexy for traumatic cyclodialysis with persisting hypotony. Report in 29 consecutive patients. Ophthalmology. 1995;102:322-333. doi:10.1016/s0161-6420(95)31021-4.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.