In SLET, a limbal tissue strip of about 2 mm (1 clock hour) is harvested from the superior limbus of the healthy donor eye. The harvested tissue is divided into 6 to 10 small pieces and placed on human amniotic membrane (HAM) laid over the cornea of the affected eye. The small pieces proliferate in vivo and regenerate the corneal epithelium.
The greatest advantage of this procedure is that it does not require a culture facility like CLET, and the amount of tissue harvested from the donor eye is smaller than in CLAu2). Since it is an autograft, systemic immunosuppression is not needed.
QWhich patients are indicated for SLET?
A
It is indicated for unilateral LSCD when the contralateral eye is healthy. Chemical and thermal burns are the most common indications2). Other indications include iatrogenic LSCD, contact lens-related LSCD, after ocular surface tumor resection, and previous failed LSCD surgery. If there is corneal stromal opacity, corneal transplantation is needed in addition to SLET.
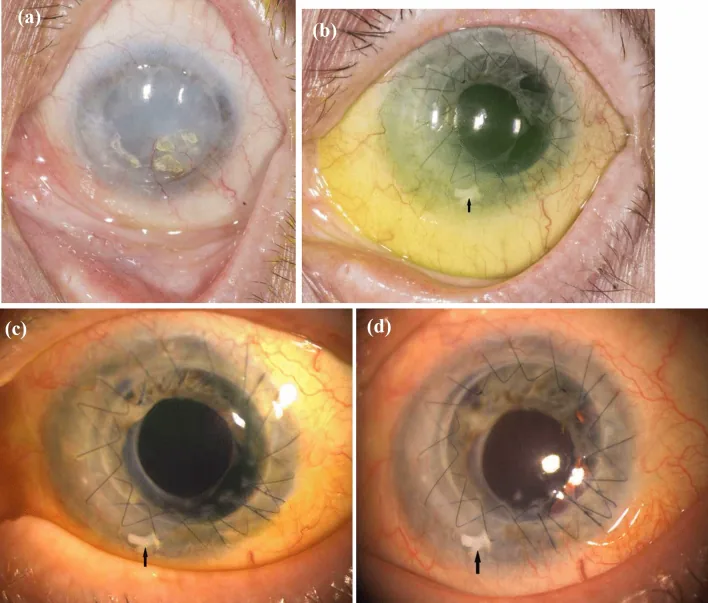
Viestenz A, Kesper C, Hammer T, et al. ALT (allogeneic limbal transplantation): a new surgical technique for limbal stem cell deficiency. International Ophthalmology. 2022 Aug 19; 42(3749):$2. Figure 3. PMCID: PMC9617846. License: CC BY.
The pre-SLET image shows diffuse corneal opacity and surface irregularity, while the postoperative image shows progression of epithelialization and restoration of transparency. The course of ocular surface reconstruction after limbal transplantation is shown in a before-and-after comparison.
LSCD is a condition in which the normal homeostasis of the corneal epithelium cannot be maintained due to dysfunction of corneal epithelial stem cells 1). Limbal stem cells reside in a specialized structure called the palisades of Vogt 1). When stem cells are damaged, the corneal epithelium is replaced by conjunctival epithelium (conjunctivalization), leading to loss of corneal transparency and decreased vision 1).
The most common cause of LSCD is chemical injury, followed by aniridia, contact lens wear, and Stevens-Johnson syndrome1). Performing corneal transplantation alone for LSCD results in recurrent epithelial breakdown and graft failure, so ocular surface reconstruction with limbal stem cell transplantation is necessary 2).
Prepare an appropriate environment for transplanted stem cells to proliferate. In cases after chemical injury, treat ocular surface inflammation before performing SLET. Use oral doxycycline, topical cyclosporine, and preservative-free artificial tears. Correct any eyelid problems preoperatively.
Anesthesia and preparation: Perform local anesthesia in both eyes, and add retrobulbar anesthesia (or sub-Tenon’s anesthesia) in the LSCD eye. Use general anesthesia in children. Preoperative instillation of 0.15% brimonidine and 5% phenylephrine reduces intraoperative bleeding.
Harvesting donor tissue: Harvest limbal tissue approximately 2 mm (1 clock hour) from the superior limbus of the healthy donor eye. Dissect 1 mm into clear cornea with a crescent knife and excise the limbal tissue. Reattach the conjunctiva with fibrin glue or sutures. Store the harvested tissue in saline.
Preparation of recipient eye: Perform a 360-degree conjunctival peritomy and carefully remove the vascular pannus on the cornea. Cover the cornea and exposed sclera with human amniotic membrane (basement membrane side up) and fix it with fibrin glue.
Placement of limbal explants: Divide the harvested limbal tissue into 6–10 small pieces on the amniotic membrane using Vannas scissors. Place the pieces in a circular pattern on the mid-peripheral cornea (epithelial side up), and apply one drop of fibrin glue on each piece. Avoid placing them over the pupillary area or the limbus.
Contact lens application: After polymerization of the fibrin glue, apply a large-diameter contact lens and administer antibiotic and steroid eye drops.
Examine the patient on postoperative day 1, week 1, and month 1, and follow up as needed thereafter. The contact lens is left in place for 7–10 days. Complete epithelialization of the corneal surface is expected by 2 weeks postoperatively, and graft transparency by 8 weeks. The amniotic membrane dissolves within a few weeks. Epithelialization and transparency occur faster in children than in adults.
The outcomes of SLET in a systematic review are as follows2).
Surgical procedure
Anatomical success rate
Functional success rate
SLET
78%
68.6%
CLAu
81%
74.4%
CLET
61.4%
53%
The outcomes of SLET and CLAu are comparable, and both are significantly better than CLET (anatomical success p=0.0048, functional success p≤0.0001) 2). The difference in functional success rates between SLET and CLAu was not statistically significant (p=0.27) 2). No serious adverse events have been reported in donor eyes 2).
QWhat is the success rate of SLET?
A
A systematic review reports an anatomical success rate (stable epithelialized corneal surface) of 78% and a functional success rate (improvement of best-corrected visual acuity [BCVA] by 2 or more lines) of 68.6% 2). These rates are comparable to CLAu (81%/74.4%) and significantly better than CLET (61.4%/53%) 2).
Subamniotic hemorrhage: The most common early postoperative complication. It can cause detachment or displacement of the amniotic membrane.
LSCD recurrence (recurrence of conjunctivalization): The most frequently reported late complication 2). Localized LSCD recurrence has been reported in 4 SLET studies 2).
Persistent corneal epithelial defect: Rarely, it can lead to perforation or infectious keratitis 2).
Infectious keratitis: May occur as a secondary infection in the postoperative immunosuppressed state 2).
Limitations include the inability to preserve donor cells as in CLET, and the cost and availability of fibrin glue and amniotic membrane may be limiting factors 2). SLET is recommended for cases with mild conjunctival involvement, while CLAu is recommended for cases with severe symblepharon2).
QHow should SLET and CLAu be used differently?
A
SLET is recommended for LSCD with mild conjunctival involvement (less symblepharon). CLAu is recommended for LSCD with severe conjunctival involvement (severe symblepharon) 2). Additionally, if the cost or availability of amniotic membrane or fibrin glue is a limiting factor, CLAu may be an option 2).
Corneal epithelial stem cells reside in the palisades of Vogt in the limbus1). These stem cells migrate centripetally while differentiating into basal epithelial cells, proliferate, move toward the surface, and eventually slough off 1). The limbus also functions as a barrier preventing conjunctival epithelium from invading the cornea1).
In LSCD, the corneal epithelium is partially or completely replaced by conjunctival epithelium 1). Even if only 7% of limbal stem cells remain, modern surgical techniques can regenerate the corneal epithelium1).
In SLET, a small amount of limbal tissue is divided into small pieces and placed on the cornea. Stem cells from each piece proliferate and migrate in vivo to regenerate the corneal epithelium. The amniotic membrane acts as a scaffold that promotes stem cell proliferation and also has anti-inflammatory effects. Fibrin glue fixes the pieces and amniotic membrane and also acts as a physiological scaffold.
Three surgical techniques for limbal stem cell transplantation (LSCT) have been developed 2). In 1989, Kenyon and Tseng reported CLAu; in 1997, Pellegrini et al. reported CLET 2). In 2012, Sangwan et al. reported SLET, simplifying the procedure by replacing the culture process of CLET with in vivo proliferation 2).
QWhy can a small amount of limbal tissue regenerate the entire corneal epithelium?
A
Limbal stem cells have self-renewal and differentiation capabilities 1). In SLET, the limbal tissue is divided into small pieces and distributed over a wide area, allowing stem cells from each piece to proliferate and migrate simultaneously to cover the corneal surface. The amniotic membrane provides an environment conducive to stem cell proliferation, enabling regeneration of the entire corneal epithelium from as little as 2 mm of limbal tissue.