Keratolimbal allograft (KLAL) is a type of ocular surface stem cell transplantation (OSST) for treating limbal stem cell deficiency (LSCD). It involves transplanting allogeneic limbal tissue attached to a corneoscleral carrier from a deceased donor to restore corneal epithelial homeostasis.
In LSCD, corneal epithelial stem cells are damaged, and the corneal epithelium is replaced by conjunctival epithelium 1). This conjunctivalization leads to loss of corneal transparency, resulting in decreased vision, scarring, and neovascularization1). Corneal transplantation alone is ineffective for treating LSCD, and repeated surface breakdown and epithelial healing failure lead to graft failure 2).
KLAL is indicated for the following cases: bilateral LSCD without a living donor; unilateral LSCD where the healthy eye is unsuitable as a donor; and LSCD with minimal conjunctival involvement, such as aniridia or contact lens-related LSCD.
Historically, Thoft reported corneal epithelial transplantation in 1984. In 1990, Turgeon and Thoft reported a modified technique including limbal tissue, which is the first recorded KLAL.
QWhat is the difference between KLAL and autograft?
A
Autografts (CLAu, SLET) harvest limbal tissue from the healthy eye for unilateral LSCD, with the advantage of no need for immunosuppression. In contrast, KLAL uses allogeneic tissue from a deceased donor, requiring systemic immunosuppression, but it can be performed in bilateral LSCD or cases where the healthy eye is unsuitable as a donor. A systematic review reported anatomical success rates of 81% for autologous CLAu and 78% for SLET2).
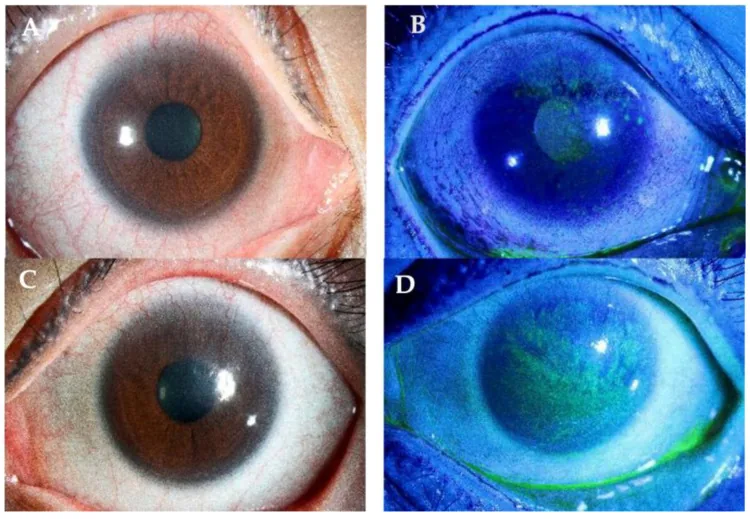
Yhu Fhei Lee, Dayna Wei Wei Yong, Ray Manotosh A Review of Contact Lens-Induced Limbal Stem Cell Deficiency 2023 Dec 5 Biology (Basel). 2023 Dec 5; 12(12):1490 Figure 3. PMCID: PMC10740976. License: CC BY.
A and C show neovascularization extending from the limbus to the cornea under fluorescein staining. B and D show pannus and superficial opacity involving the visual axis, indicating the extent of limbal stem cell damage.
Patients with LSCD primarily complain of decreased visual acuity. This is due to loss of corneal transparency caused by conjunctivalization and scarring of the cornea. If persistent corneal epithelial defects occur, eye pain may be present. Photophobia and tearing are also observed.
In mild LSCD, fluorescein staining reveals whorl-like epitheliopathy 1). In moderate cases, superficial corneal neovascularization and peripheral pannus appear 1). In severe cases, total conjunctivalization replaces the entire cornea with conjunctival epithelium 1).
In the severity classification of LSCD, based on clinical grading, it is classified as mild (2–4 points), moderate (5–7 points), and severe (8–10 points) 1). Basal epithelial cell density is 9,252 cells/mm² in control eyes, whereas it decreases to 2,821 cells/mm² in severe LSCD eyes 1).
LSCD occurs when limbal stem cells are damaged. The most common cause is aniridia (30.9%), followed by chemical burns (20.6%), contact lens wear (16.8%), and SJS (10.4%) 1). In unilateral cases, chemical burns are the most common cause 1).
Glaucoma surgery is a risk factor for LSCD1). Direct mechanical trauma from trabeculectomy or aqueous shunt surgery damages limbal stem cells1). Concurrent use of antimetabolites (mitomycin C, 5-FU) also affects the limbal microenvironment 1). It has been reported that 35% of LSCD patients have glaucoma or ocular hypertension1).
In chemical burns, the corneal epithelial stem cells located in the limbal corneoscleral junction are damaged. Loss of the palisades of Vogt reflects the extent of corneal epithelial stem cell damage.
The diagnosis of LSCD is based on a combination of clinical findings and imaging tests 1).
Clinical Tests
Slit-lamp microscopy: Direct observation of the loss of Vogt’s palisades 1). Fluorescein staining evaluates the extent of vortex keratopathy or conjunctivalization 1).
Impression cytology: Collection of ocular surface epithelium using a cellulose acetate filter 1). The presence of goblet cells indicates conjunctivalization 1). It is considered a diagnostic criterion for LSCD, but sample quality varies 1).
Imaging Tests
In vivo confocal microscopy: Allows observation of morphological differences between corneal and conjunctival epithelium 1). Corneal epithelium consists of large polygonal flattened cells, while conjunctival epithelium has cuboidal cells with highly reflective cytoplasm 1).
Anterior segment OCT (AS-OCT): Enables non-contact rapid assessment 1). It can evaluate the extent of conjunctivalization and changes in epithelial thickness.
Performed under general or retrobulbar anesthesia. A 360-degree limbal conjunctival incision (peritomy) is made, and fibrovascular pannus and abnormal epithelium are removed from the corneal surface. The central cornea is excised from two donor corneoscleral rims to create four crescent-shaped limbal grafts. The posterior half of each crescent is removed by lamellar dissection, and typically three crescents are placed around the recipient cornea. They are secured with 10-0 nylon sutures and tissue adhesive.
Donor tissue selection criteria include young donors under 60 years, minimal time from death to preservation, and transplantation within 5 days of death.
Systemic immunosuppression is essential for long-term graft survival after KLAL. The Cincinnati OSSTP protocol starts oral tacrolimus 4 mg twice daily and MMF 1 g twice daily 1–2 weeks before surgery. Postoperatively, oral prednisone 1 mg/kg/day is added and tapered over 1–3 months. In patients with stable ocular surface, tacrolimus is gradually tapered starting 12–18 months after surgery, and MMF starting 3 years after surgery.
Stable ocular surface: Achieved in 73–77% of patients under appropriate triple immunosuppression. Reported with a mean follow-up of 4.5–4.7 years.
Classification of graft failure: primary failure (epithelialization failure within 1 week postoperatively), partial failure (conjunctivalization mixed with healthy epithelium), total failure (recurrence of total LSCD), and late failure (due to chronic rejection).
Risk factors for failure: keratinization, dry eye, symblepharon, chronic inflammation, and history of rejection.
Comparison of autologous LSCT techniques
CLAu (conjunctival limbal autograft): anatomical success rate 81%, functional success rate 74.4%2). First reported by Kenyon and Tseng in 19892).
CLET (cultured limbal epithelial transplantation): anatomical success rate 61.4%, functional success rate 53%, inferior to CLAu and SLET2).
QHow long is immunosuppression needed?
A
Systemic immunosuppression is usually tapered gradually: tacrolimus starting at 12–18 months postoperatively, and MMF starting at 3 years postoperatively. If the ocular surface is stable and there is no history of rejection, it may eventually be discontinued. However, if there is a history of rejection, low-dose immunosuppression must be continued indefinitely. Collaboration with organ transplant specialists is recommended.
QDoes vision recover after KLAL?
A
The primary goal of KLAL is to establish a stable ocular surface, not direct visual improvement. However, after the corneal surface stabilizes, additional optical corneal transplantation (PKP or DALK) can be expected to restore vision. In one reported case of KLAL followed by DMAK + allo-SLET, corrected visual acuity improved from 20/200 to 20/403).
Limbal stem cells reside in the palisades of Vogt in the basal layer of the limbus1). These stem cells migrate centripetally, first differentiating into basal epithelial cells, then proliferating and migrating toward the surface before shedding1). The limbus also functions as a barrier against conjunctival invasion onto the cornea1).
In LSCD, damage to limbal stem cells leads to replacement of corneal epithelium by conjunctival epithelium, resulting in loss of corneal transparency. If as little as 7% of limbal stem cells remain, modern surgical techniques can regenerate the corneal epithelium. 1)
In long-term ocular diseases, the combined action of inflammatory cytokines and mucous membrane pemphigoid alters the microenvironment of limbal stem cells1). In LSCD associated with bullous keratopathy, epithelialization takes about 6 days in eyes without corneal neovascularization, whereas it takes about 29 days in eyes with neovascularization1).
Corneal epithelium and conjunctival epithelium are morphologically different 1). Normal corneal epithelium consists of large polygonal flattened cells, with a basal layer having low-reflectivity cytoplasm and distinct borders 1). Conjunctival epithelium is cuboidal with more highly reflective cytoplasm and contains goblet cells 1). Cytokeratin 3 is specific to corneal epithelium, and cytokeratin 19 is specific to conjunctival epithelium 1).
As a salvage after KLAL failure, the combination of Descemet membrane anterior keratoplasty (DMAK) using decellularized Descemet membrane and allogeneic simple limbal epithelial transplantation (allo-SLET) has been reported 3). Descemet membrane is more resistant to degradation compared to human amniotic membrane (HAM); it withstands high-concentration collagenase immersion for over 24 hours, whereas HAM degrades within 30 minutes 3).
Limbal stem cells cultured on Descemet membrane have been reported to show better expression of stem cell markers (ABCG2, p63) compared to those on HAM 3). In a case of LSCD associated with autoimmune polyglandular syndrome, after KLAL rejection followed by DMAK + allo-SLET, corrected visual acuity improved from 20/200 to 20/40, and no recurrence of epithelial defect was observed for 1.5 years 3).
Descemet membrane has advantages in transparency, durability, and as a substrate for limbal stem cell culture, and is promising as a salvage method after KLAL failure. However, further investigation is needed regarding long-term efficacy and immune response. 3)
Progress has also been made in the diagnosis of LSCD1). With improved accuracy of in vivo confocal microscopy and AS-OCT, objective assessment of LSCD severity and monitoring of treatment effects are improving 1). In aniridia, advances in genetic analysis may contribute to prognosis prediction and management 1).