Optic disc drusen (ODD) are calcified deposits that accumulate within the optic nerve head. They consist of refractive calcified material composed of mucoproteins and mucopolysaccharides, and are thought to result from impaired axoplasmic transport leading to deposition of calcified aggregates of extracellular material in the optic nerve head2). There are two types: superficial, where granules are visible on the disc surface, and buried, which are not visible from the surface.
ODD are congenital, but often not apparent in early childhood. They are mostly discovered incidentally during fundus examinations for health checkups or other diseases. Prevalence varies by detection method: about 0.37% by ophthalmoscopy, 0.12% by fundus photography, but 2.21% by spectral-domain OCT with enhanced depth imaging (EDI)4). There is no sex predilection; over 70% of cases are bilateral but often asymmetric2).
ODD are a common cause of pseudopapilledema, and buried type in particular can be difficult to differentiate from papilledema. Previously considered a benign static condition, recent studies show that visual field abnormalities occur in over 70% of patients and progress slowly, leading to its recognition as a chronic progressive optic neuropathy.
QAre optic disc drusen and retinal drusen the same?
A
Although the names are similar, they are different diseases. Optic disc drusen (ODD) are calcified deposits within the optic nerve head and differ completely from retinal drusen on Bruch’s membrane, which are precursor lesions of age-related macular degeneration, in terms of location, composition, and clinical significance. ODD is a congenital optic nerve disease and is unrelated to age-related macular degeneration.
QAre optic disc drusen hereditary?
A
Autosomal dominant inheritance with incomplete penetrance is suspected. If there is a family history of ODD, an eye examination is recommended. A high rate of bilaterality is also characteristic.
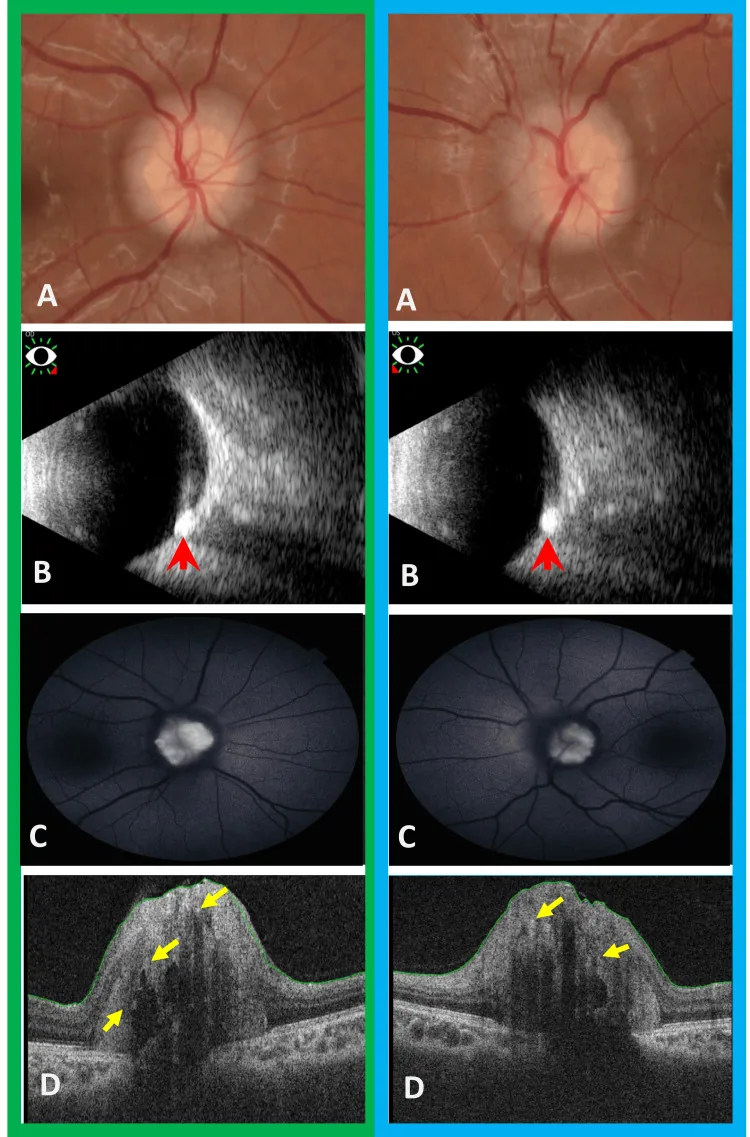
Alkhayat MI, et al. Chiari Malformation Type I With Concurrent Bilateral Optic Disc Drusen: Is Follow-up Necessary?. Cureus. 2024. Figure 2. PMCID: PMC11298954. License: CC BY.
White, irregular drusen are seen on the optic nerve head of both eyes. Ultrasound shows high echogenicity and posterior shadowing, and OCT shows hyporeflective cavities and hyperreflective spots corresponding to buried drusen, illustrating the main clinical and diagnostic findings.
The course of ODD is usually asymptomatic. Visual field abnormalities progress slowly, so in many cases patients are unaware of visual field defects.
Transient visual obscuration: occurs in about 9% of patients 2)
Visual field abnormalities: patterns of enlarged blind spot, arcuate scotoma, and peripheral depression, appearing along the course of retinal nerve fibers 2)
Sudden vision loss: rarely, patients may experience acute vision loss when complicated by NA-AION or CNVM (see Treatment section)
Visual field abnormalities take the following forms.
Optic nerve fiber bundle defect: Arcuate visual field defect along the nerve fiber course
Mariotte blind spot enlargement: Enlargement of the physiological blind spot
Peripheral visual field constriction: Concentrically progressive visual field narrowing
Horizontal hemianopia: Rare but reported
Pattern
Characteristics
Blind spot enlargement
Most common
Arcuate scotoma
Along the optic nerve fiber course
Peripheral visual field constriction
Appears in advanced cases
All of these progress slowly, so even if visual field abnormalities are present at the first visit, patients often have no subjective symptoms. The frequency of visual field defects is reported to be about 73% in the superficial type and about 36% in the buried type, and the larger the drusen volume, the stronger the visual field impairment tends to be5). Visual field constriction progresses at a rate of approximately 1.6% per year. The main cause of visual field impairment is direct axonal compression of optic nerve fibers by drusen2).
Small optic disc: optic disc drusen are often associated with small optic discs
Peripapillary CNVM: rarely occurs and can cause sudden vision loss
NA-AION: consider when sudden visual field defect or vision loss is noticed
If sudden visual field defect or vision loss is noticed, it is thought to be due to optic disc ischemia. This mechanism is similar to that of ischemic optic neuropathy (NAION), and urgent evaluation is necessary.
QCan optic disc drusen cause blindness?
A
The visual prognosis is usually good. However, there is approximately 1.6% per year progression of visual field constriction, and rarely, sudden vision loss can occur with NA-AION or CNVM. Regular examinations are important.
As the mechanism of ODD formation, calcification secondary to axonal transport impairment is widely accepted7).
Axonal transport is obstructed anterior to the lamina cribrosa of the optic disc
Intracellular organelles such as mitochondria accumulate within the optic disc
Substances such as mucopolysaccharides and calcium phosphate are deposited
These calcify to form drusen
This process begins in early childhood and calcification progresses with age. In early childhood, drusen often exist as buried drusen, and become visible as superficial drusen in adolescence to adulthood.
Small optic disc (narrow scleral canal, crowded optic disc): Optic nerve fibers pass through the lamina cribrosa in a crowded state, making axonal transport impairment more likely. The frequent association of small optic disc with optic disc drusen supports this mechanism2)
Absence of optic cup: A characteristic anatomical finding of ODD, related to the pathology
ODD is often bilateral, and familial cases have been reported. An autosomal dominant inheritance pattern with incomplete penetrance has been suggested, but specific gene mutations have not yet been identified. Genetic predisposition may contribute to small optic disc formation or vulnerability of axonal transport.
The diagnosis of ODD involves a combination of multiple tests. In particular, diagnosing buried drusen and differentiating them from papilledema are important clinical challenges. The Optic Disc Drusen Studies (ODDS) Consortium has established consensus criteria for ODD diagnosis using EDI-OCT (including areas of signal loss anterior to the lamina cribrosa and internal hyperreflective foci), which are widely referenced as the current standard diagnostic approach.
The basic findings are absence of optic cup and elevation of the optic disc. In superficial drusen, diagnosis can be made by the presence of white particles on the disc surface.
Using red-free light (green filter) to take fundus photographs makes drusen appear glittering and bright. This is useful for confirming superficial drusen.
Superficial type: Clearly visualized as hyperautofluorescence
Buried type: Autofluorescence can be detected, useful for detecting buried drusen not visible on fundus examination
Differential diagnosis: Since congested optic disc does not show autofluorescence, it is directly useful for differentiation.
OCT (EDI-OCT)
Findings: Identified as a hyporeflective ovoid structure within the optic nerve head.
Significance: Shows higher detection sensitivity for buried drusen compared to conventional OCT or B-mode ultrasound, and is currently considered the most sensitive diagnostic modality.
RNFL assessment: Useful for detecting early thinning of the retinal nerve fiber layer. The localization of visual field defects matches the distribution of RNFL defects 3).
Ultrasound (B-mode/A-mode)
Findings: Detects high-intensity echoes (high-amplitude spikes) at calcified sites.
Features: The signal is maintained even when gain is reduced.
Significance: Non-invasive and repeatable. Useful as an alternative when CT is difficult (e.g., in children).
Fluorescein angiography (FA): In ODD, dye leakage from the optic disc is generally absent. In contrast, congested optic disc or optic disc edema shows fluorescein leakage. The presence of only peripapillary staining without leakage suggests pseudopapilledema (ODD). If there is early capillary dilation and late leakage on FA, it suggests CNVM.
CT: Superior to MRI for detecting drusen. When slicing through the optic nerve head, calcifications appear as high-attenuation areas. It is one of the most reliable imaging tests for differentiating from congested optic disc.
PHOMS assessment: Evaluation of peripapillary hyperreflective ovoid mass-like structures (PHOMS) on OCT contributes to improved diagnostic accuracy of pseudopapilledema.
Differentiation from congested optic disc (most important)
ODD is also important in the differential diagnosis of glaucoma.
QHow is buried optic disc drusen diagnosed?
A
Buried drusen are not visible on fundus examination alone, so fundus autofluorescence (FAF) is the first choice. Autofluorescence corresponding to the drusen site provides diagnostic evidence. CT for calcification, B-mode ultrasound, and EDI-OCT are useful for confirmation. The absence of dye leakage from the optic disc on fluorescein angiography is also an important finding to differentiate from papilledema.
QA child was told during a health check that the optic disc is swollen. Could it be drusen?
A
In children with bilateral optic disc edema-like findings, ODD is a differential diagnosis. It is important to check for calcification using B-mode ultrasound or OCT to distinguish from true optic disc edema. Neurological evaluation should be considered if necessary.
Regular visual field testing and imaging evaluation are the core of management.
Visual field testing: Automated perimetry using Humphrey or similar devices is performed regularly to detect progression of visual field defects.
OCT-RNFL: Longitudinal measurement of retinal nerve fiber layer thickness allows early detection of thinning (irreversible neuronal loss).
Fundus photography: Records and compares changes in optic disc appearance.
The interval between visits varies depending on disease severity and degree of visual field abnormality, but regular follow-up is essential. No effective treatment for visual field defects has been established; in some cases, intraocular pressure-lowering medications may be considered.
In a case report by Markan et al., multimodal imaging was performed in an early teenage boy with peripapillary CNVM associated with ODD. Left eye BCVA was 6/60, and he had been misdiagnosed with optic neuritis at another hospital and treated with steroids. After three anti-VEGF injections, subretinal fluid resolved, and BCVA improved to 6/9 at 3 months.
Treatment options for CNVM complication are as follows:
Anti-VEGF therapy: Efficacy has been shown in case reports.
Consider anti-VEGF therapy, PDT, or laser photocoagulation
QIs treatment necessary if diagnosed with drusen?
A
There is no effective treatment for drusen themselves. Management mainly addresses complications (e.g., CNVM). Regular visual field testing and observation of optic disc morphology changes are important. Seek immediate medical attention if sudden vision loss or visual field abnormalities occur.
6. Pathophysiology and Detailed Mechanism of Onset
The formation of ODD results from a combination of anatomical characteristics of the optic disc and impaired axonal transport. A congenitally small and crowded optic disc is a prerequisite for formation 2).
When the optic nerve passes through the lamina cribrosa to exit the eye, all axons of retinal ganglion cells pass through this narrow opening (scleral canal). In individuals with a small scleral canal, nerve fibers become more densely packed.
Transport impairment: In a densely packed axonal environment, axonal transport (transport of materials and energy within nerve fibers) is prone to obstruction anterior to the lamina cribrosa
Accumulation of intracellular substances: When transport is stalled, intracellular organelles such as mitochondria and endoplasmic reticulum, as well as mucopolysaccharides, accumulate within the optic disc
Progression of calcification: Calcium phosphate deposits on the accumulated substances, gradually calcifying to form drusen7)
As drusen enlarge with age, mechanical compression of optic nerve fibers occurs, leading to progressive visual field defects 2). The mechanism of visual field defect development is as follows.
Mechanical compression: Direct compression of optic nerve fibers by drusen
Ischemia: Impaired blood flow to the optic disc
Axonal flow impairment: Chronic inhibition of axonal transport
The size and location of drusen do not always correlate with visual field changes. The mechanism of CNVM (peripapillary choroidal neovascular membrane) development is presumed to involve effects on choroidal vessels at the ODD site and disruption of peripapillary vascular structures.
This calcification process is thought to begin shortly after birth. In early childhood, calcifications are small and buried within the optic disc, making them inconspicuous externally. From adolescence to adulthood, calcification progresses, and drusen become exposed on the disc surface, visible as superficial drusen. The absence of optic cup excavation is interpreted as being due to compression of anatomical space by intra-disc drusen formation, and is one of the characteristic fundus findings of ODD.
ODD was once considered a static benign lesion, but since visual field abnormalities are found in over 70% of cases and progress slowly, it is now regarded as a chronic progressive optic nerve disease. Continuous axonal compression and local ischemia are thought to cause gradual loss of optic nerve fibers, increasing the importance of long-term visual field monitoring.
7. Latest Research and Future Perspectives (Research Stage Reports)
Visualization and shape evaluation of optic disc drusen using enhanced depth imaging OCT (EDI-OCT) have developed rapidly in recent years 1). Quantification of drusen depth, volume, and number is becoming possible, and it is expected to become a tool for progression monitoring in the future. The spread of OCT has also improved detection accuracy for buried drusen, and the introduction of the concept of PHOMS (peripapillary hyperreflective ovoid mass-like structures) is further improving diagnostic accuracy for pseudopapilledema6).
Multimodal imaging combining fundus autofluorescence, OCT, OCT-A, FA, and ultrasound (USG) is useful for comprehensive evaluation of ODD-related complications. In particular, OCT-A is useful for detecting peripapillary choroidal neovascular membranes (CNVM) and contributes to identifying cases missed by FA alone.
Movement toward international unification of terminology and classification
Diagnostic criteria and terminology for ODD have varied by institution and country. International consensus formation (e.g., ODDS Consortium) is progressing, and unification of diagnostic criteria is thought to contribute to improved accuracy of future research.
Case reports have shown the efficacy of anti-VEGF therapy for CNVM associated with ODD, and accumulation of evidence is expected. Although the number of cases is small and long-term outcomes are unknown, it is being considered as a treatment option.
Long-term prospective studies on the rate of progression and predictors of visual field defects in the natural history of ODD are lacking. Research examining the relationship between drusen size, location, number, and visual field prognosis is an important future issue 5).
Association with NA-AION-like Acute Optic Nerve Ischemia
Acute optic nerve ischemia associated with ODD (especially in patients under 50 years of age) has been reported to show a non-arteritic anterior ischemic optic neuropathy (NA-AION)-like pathology 2). It has been suggested that structural narrowing within the optic disc may increase the risk of ischemic onset, and elucidating risk factors and establishing preventive strategies remain future challenges.
QWhen should one see an ophthalmologist for optic disc drusen?
A
Since it is usually asymptomatic, regular ophthalmic check-ups are the basis. If already diagnosed, it is important to undergo visual field tests at intervals instructed by the attending physician. If you notice sudden vision loss, rapid changes in visual field, flashes, or photopsia, promptly consult an ophthalmologist.
Malmqvist L, Bursztyn L, Costello F, et al. The Optic Disc Drusen Studies Consortium recommendations for diagnosis of optic disc drusen using optical coherence tomography. J Neuroophthalmol. 2018;38(3):299-307. PMID: 29095768.
Costello F, Rothenbuehler SP, Sibony PA, Hamann S; Optic Disc Drusen Studies Consortium. Diagnosing optic disc drusen in the modern imaging era: a practical approach. Neuroophthalmology. 2020;45(1):1-16. PMID: 33762782; PMCID: PMC7946029.
Wandji BN, Dugauquier A, Ehongo A. Visual field defects and retinal nerve fiber layer damage in buried optic disc drusen: a new insight. Int J Ophthalmol. 2022;15(10):1641-1649. PMID: 36262850; PMCID: PMC9522567.
Mukriyani H, Malmqvist L, Subhi Y, Hamann S. Prevalence of optic disc drusen: a systematic review, meta-analysis and forecasting study. Acta Ophthalmol. 2024;102(1):15-24. PMID: 37144704.
Lee KM, Woo SJ, Hwang JM. Factors associated with visual field defects of optic disc drusen. PLoS One. 2018;13(4):e0196001. PMID: 29708976; PMCID: PMC5927402.
Sibony PA, Kupersmith MJ, Kardon RH. Optical Coherence Tomography Neuro-Toolbox for the Diagnosis and Management of Papilledema, Optic Disc Edema, and Pseudopapilledema. J Neuroophthalmol. 2021;41(1):77-92. doi:10.1097/WNO.0000000000001078. PMID:32909979; PMCID:PMC7882012.
Liu X, Yan Y. Advances in origin, evolution, and pathogenesis of optic disc drusen: a narrative review. Indian J Ophthalmol. 2025;73(5):637-647. PMID: 40272291; PMCID: PMC12121874.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.