Optic Perineuritis (OPN)

Optic Perineuritis
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is Optic Perineuritis?
Section titled “1. What is Optic Perineuritis?”Optic perineuritis (OPN) is a type of orbital inflammatory disease in which inflammation is confined to the meninges (sheath) of the optic nerve. In 1883, Edmunds & Lawford first reported inflammatory infiltration around the optic nerve in pathological specimens.
There are two conceptual perspectives on OPN. The classical concept refers to bilateral papilledema caused by meningitis due to syphilis or sarcoidosis. The newer concept refers to inflammation confined to the optic nerve sheath, showing a ring-like hyperintensity on MRI, without visual impairment other than enlargement of the Mariotte blind spot.
Classification is as follows:
- Primary (idiopathic) OPN: No underlying disease identified. Accounts for the majority.
- Secondary OPN: Associated with underlying diseases such as systemic inflammation, infection, or malignancy.
Epidemiology
Section titled “Epidemiology”The mean age of onset is 40–60 years (range 15–85 years), with a slight female predominance, but a definitive sex difference has not been established.
Q
What is the difference between optic perineuritis and optic neuritis?
A
Optic neuritis (ON) is a disease in which inflammation occurs in the optic nerve itself (axons and myelin sheath), often demyelinating and associated with MS. Optic perineuritis (OPN) is inflammation confined to the sheath (meninges) surrounding the optic nerve, showing enhancement around the nerve sheath on MRI. OPN is characterized by preserved central vision, lower frequency of RAPD, rapid response to steroids, and tendency to relapse upon tapering, making clinical differentiation from ON important.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”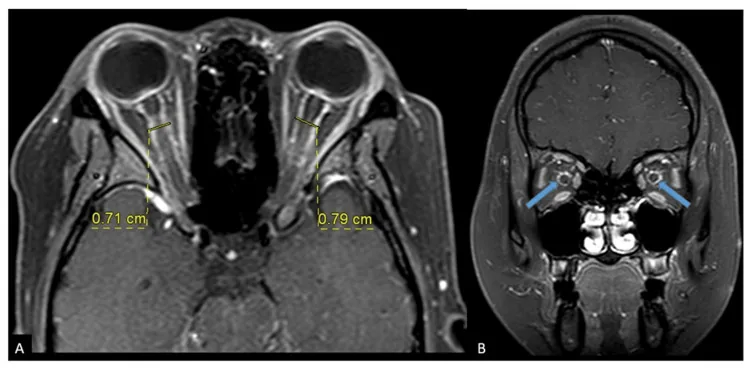
A Case Report of Bilateral Optic Perineuritis With Idiopathic Intracranial Hypertension: Challenges in Diagnosis and Management. Cureus. 2024 Feb 27; 16(2):e54692. Figure 4. PMCID: PMC10960579. License: CC BY.
(A) Axial T1 post Gadolinium shows increase bilateral optic nerve sheath diameter. (B) Coronal T1 post Gadolinium shows circumferential thickening of bilateral optic nerve sheath with enhancement.
Subjective Symptoms
Section titled “Subjective Symptoms”- Eye pain / pain on eye movement: Most common subjective symptom. Often more severe and persistent than typical ON.
- Vision loss: Ranges from asymptomatic to severe. May report blurred vision, scotomas (“spots”).
- Onset: Slowly progressive over weeks (slower than ON which progresses over days).
- Orbital symptoms: Rarely, proptosis or limited eye movement.
Clinical Findings
Section titled “Clinical Findings”- Optic disc edema: Present in most patients. Some cases have normal discs.
- Central vision: Relatively preserved. However, some cases may have severe loss (NLP to CF).
- Color vision / RAPD: Abnormalities are infrequent or mild.
- Visual field defects: Various patterns including arcuate scotoma, paracentral scotoma, central scotoma, peripheral sparing, horizontal hemianopia, enlarged Mariotte blind spot.
- Orbital signs: Ptosis, ophthalmoplegia, proptosis may be present.
- Mostly unilateral but bilateral cases reported. 1)5)7)
- In cases with polyarteritis nodosa (PAN), paroxysmal alternating blindness has been reported. 5)
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The majority of OPN cases are idiopathic. In secondary OPN, the following underlying diseases are identified.
Systemic Inflammatory Diseases
Section titled “Systemic Inflammatory Diseases”- Sarcoidosis: One of the main causes of classic OPN
- IgG4-related disease
- Granulomatosis with polyangiitis (GPA)
- Giant cell arteritis
- Behçet’s disease / SLE
- Inflammatory bowel disease (including Crohn’s disease)8)
- Polyarteritis nodosa (PAN)5)
Infectious Diseases
Section titled “Infectious Diseases”- Tuberculosis2)7) · Syphilis · HSV · VZV · COVID-191)
Autoimmune / Antibody-Related
Section titled “Autoimmune / Antibody-Related”- MOGAD (MOG antibody-associated disease): A major differential diagnosis alongside sarcoidosis. MRI findings show tram-track enhancement.1)
Malignancy
Section titled “Malignancy”- Leukemia/lymphoma (primary or metastatic)3)
Drug-induced/Iatrogenic
Section titled “Drug-induced/Iatrogenic”- Immune checkpoint inhibitors (nivolumab): May develop as an irAE.4)
- After flow diverter placement6)
TB-IRIS
Section titled “TB-IRIS”- Immune reconstitution inflammatory syndrome during anti-tuberculosis treatment (TB-IRIS)7)
Q
If diagnosed as idiopathic, are additional tests necessary?
A
Even if diagnosed as idiopathic OPN, systemic evaluation is recommended because an underlying disease may be present. Main tests include syphilis serology, ACE (to rule out sarcoidosis), ANCA, IgG4, MOG antibodies, AQP4 antibodies, ESR, CRP, and chest X-ray. Identifying an underlying disease can also help prevent recurrence through treatment of the primary condition.
4. Diagnosis and Testing Methods
Section titled “4. Diagnosis and Testing Methods”Imaging Diagnosis
Section titled “Imaging Diagnosis”MRI is the cornerstone of diagnosis. The following findings are confirmed on gadolinium-enhanced, fat-suppressed T1-weighted images.
- Tram-track sign: Axial view showing double linear enhancement of the optic nerve sheath.
- Doughnut sign: Coronal view showing ring-like enhancement around the optic nerve. STIR coronal view is also useful.6)
In differentiating from ON, it is important that in ON the optic nerve itself enhances, whereas in OPN the area around the optic nerve sheath enhances. However, the tram-track sign is not specific to OPN and can also appear in optic nerve sheath meningioma, sarcoidosis, and leukemia. CT is insufficient for diagnosis due to poor soft tissue resolution.
The main differentiating points between OPN and ON are shown below.
Typical Optic Neuritis (ON)
Onset speed: Rapidly progressive over days
Central visual acuity: Prone to decrease
RAPD: Frequently positive
MRI enhancement site: Optic nerve itself (axons and myelin enhance)
Steroid response: Promotes recovery but spontaneous remission occurs
MS-related: Yes (50% of idiopathic ON convert to MS within 15 years)
Ophthalmic and neurophysiological tests
Section titled “Ophthalmic and neurophysiological tests”- Visual acuity and visual field tests: Evaluate various defect patterns using Humphrey and Goldmann perimetry.
- Color vision (Ishihara) and pupillary examination (RAPD): Assess, though less frequently performed.
- Optical coherence tomography (OCT): Can confirm retinal nerve fiber layer thickening in the acute phase and thinning in the chronic phase. 1)7)
Blood and cerebrospinal fluid tests
Section titled “Blood and cerebrospinal fluid tests”- No specific test for ON exists. The following tests are performed for differential diagnosis and etiological investigation.
- Syphilis serology, ACE, ANCA, IgG4, MOG antibody, AQP4 antibody
- ESR, CRP
- If no underlying disease is identified, lumbar puncture is performed to rule out CNS infection or malignancy. Classic ON may show pleocytosis in CSF.
Differential diagnosis
Section titled “Differential diagnosis”- Demyelinating optic neuritis, MOG-ON, AQP4-ON
- Orbital inflammatory syndrome (idiopathic, IgG4-related, sarcoidosis)
- Infections (tuberculosis, syphilis, Lyme disease, bartonellosis)
- Tumors (meningioma, leukemia, lymphoma, metastasis)
- Secondary papilledema associated with posterior scleritis or uveitis
- Choked disc, ischemic optic neuropathy, diabetic papillopathy, papillitis
5. Standard Treatment
Section titled “5. Standard Treatment”The basic treatment strategy is treatment of the underlying disease and follow-up observation. If treatment of the underlying disease is effective, visual function usually does not decline.
Systemic Corticosteroid Therapy
Section titled “Systemic Corticosteroid Therapy”High-dose steroids are the first-line treatment. A characteristic feature is a more rapid response than in optic neuritis, with symptom relief within hours to one day after starting treatment.
- Acute phase (steroid pulse therapy): Methylprednisolone 1,000 mg/day intravenously for 3 days4)5)6)7)
- Maintenance phase: Oral prednisolone (starting at 1 mg/kg/day with gradual tapering)7)
The relationship between dose and recurrence rate is an important clinical consideration.
| Oral prednisolone dose | Recurrence rate |
|---|---|
| Low dose (30–40 mg/day) | Higher recurrence rate than high-dose group |
| High dose (60–80 mg/day) | Lower recurrence rate than low-dose group |
Treatment of the underlying disease in secondary OPN
Section titled “Treatment of the underlying disease in secondary OPN”- Tuberculosis cases: Antituberculosis drugs (ofloxacin, isoniazid, rifampicin, pyrazinamide) + dexamethasone (CNS TB treatment regimen) 2)
- PAN cases: Intravenous cyclophosphamide (1000 mg × 7 doses) + high-dose steroids + azathioprine 150 mg 5)
- Malignancy cases: Chemotherapy (e.g., intrathecal methotrexate) 3)
- Immune checkpoint inhibitor-related cases: Discontinuation of the causative drug + steroids 4)
Refractory cases and other options
Section titled “Refractory cases and other options”- Radiation therapy / immunosuppressants (azathioprine): Used in steroid-resistant cases.
- Indomethacin: Reported to be effective in a case by Purvin et al.
- Possibility of spontaneous remission: If visual function is preserved and pain is mild, observation may be an option. More than 7 cases of spontaneous remission have been reported in the literature. 8)
Follow-up
Section titled “Follow-up”Regularly assess visual acuity, visual field, color vision, pupils, and fundus. If symptoms do not persist, repeat imaging is usually unnecessary, but monitoring for recurrence is important.
Q
Will it recur if I stop steroids?
A
In OPN, relapse is common when tapering steroids, and abrupt discontinuation should be avoided. For oral prednisolone, the low-dose (30–40 mg/day) group is known to have a higher recurrence rate than the high-dose (60–80 mg/day) group, so gradual tapering is recommended. Spontaneous remission has been reported in the literature, but only in selected cases where visual function is preserved and pain is mild.
Q
Can it heal on its own without treatment?
A
In cases where visual function is preserved and eye pain is mild, spontaneous remission has been reported with observation alone. More than six cases of spontaneous remission have been confirmed in the literature, including a case with Crohn’s disease where pain resolved in two weeks and complete remission occurred in three months. 8) However, if vision loss is progressive or an underlying disease is suspected, active treatment is necessary, and choosing observation on your own is dangerous.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”The essence of OPN is immune-mediated inflammation of the meninges surrounding the optic nerve.
Pathological Changes
Section titled “Pathological Changes”- Thickening and inflammatory infiltration of the meninges around the optic nerve (polymorphonuclear leukocytes → lymphocyte infiltration) → fibrosis
- Some cases show granulomatous inflammation or local necrosis
- In cases with visual impairment, vasculitic changes causing demyelination or infarction of the optic nerve are observed
- Inflammation is mainly confined to the nerve sheath, but the optic nerve axons are also affected to varying degrees
Mechanisms by Underlying Disease
Section titled “Mechanisms by Underlying Disease”In MOGAD-associated OPN, humoral mechanisms mediated by MOG-IgG antibodies are central. Autoantibody binding to surface myelin triggers complement activation and cell damage. In post-COVID-19 MOGAD, cytokine storm-induced disruption of the blood-brain barrier (BBB) is thought to allow low-titer antibodies (1:20) to enter the CNS. Release of IL-1β, IL-6, TNF, and IFN-1, along with apoptosis of brain microvascular endothelial cells, is involved in the pathology. 1)
In TB-IRIS-associated OPN, during immune reconstitution due to anti-tuberculosis treatment, a Th1-dominant excessive immune response to Mycobacterium tuberculosis (MTB) triggers inflammation around the optic nerve. 7)
In IBD-associated OPN, upregulation of systemic inflammatory cytokines and antigen cross-reactivity are thought to be involved. 8)
Immune checkpoint inhibitor-related OPN involves the release of immune checkpoints due to PD-1 inhibition, which triggers perioptic nerve inflammation as an immune-related adverse event (irAE). 4)
7. Latest Research and Future Perspectives (Research-stage Reports)
Section titled “7. Latest Research and Future Perspectives (Research-stage Reports)”MOGAD-related OPN
Section titled “MOGAD-related OPN”MOGAD is increasingly recognized as an important cause of OPN. It is considered a major differential diagnosis alongside sarcoidosis.
Leitão et al. (2023) reported a 56-year-old man who developed bilateral MOGAD-OPN after severe COVID-19 infection. He was positive for MOG-IgG at a low titer of 1:20, with elevated inflammatory markers (ESR 42 mm/h, CRP 8.2 mg/dL). Visual fields improved after methylprednisolone pulse therapy (1,000 mg × 3 days), and MOG antibodies became negative after 6 months. 1)
Immune Checkpoint Inhibitor (ICI)-related OPN
Section titled “Immune Checkpoint Inhibitor (ICI)-related OPN”Cases of OPN as an irAE have been reported, suggesting potential resistance to steroid therapy.
Takada et al. (2021) reported a 54-year-old man who developed right eye visual acuity decline (20/2000) after the 7th cycle of nivolumab therapy for non-small cell lung cancer. MRI showed tram-track sign and doughnut sign, leading to a diagnosis of OPN. Two courses of steroid pulse therapy resulted in poor visual field improvement. This is the first reported case of OPN as an irAE. 4)
OPN after Flow Diverter Placement
Section titled “OPN after Flow Diverter Placement”OPN has been reported as a new complication after endovascular treatment.
Tanaka et al. (2022) reported two cases (49-year-old and 57-year-old women) who developed OPN after flow diverter placement for internal carotid artery ophthalmic artery aneurysms. Postoperative visual field defects appeared, and MRI STIR coronal sections showed a doughnut sign. Improvement was achieved with steroid pulse therapy. The importance of preoperative STIR coronal evaluation was emphasized. 6)
Possibility of Spontaneous Remission
Section titled “Possibility of Spontaneous Remission”OPN was traditionally considered to require treatment in all cases, but in some cases, observation may be an option.
Pickel et al. (2022) reported a case of spontaneous remission of right optic perineuritis in a 28-year-old woman with Crohn’s disease. She chose observation without treatment while maintaining visual acuity of 20/20, achieving pain resolution in 2 weeks and complete remission in 3 months. A literature review identified 6 cases of spontaneous remission, concluding that observation may be an option in cases with preserved visual function and mild pain. 8)
Tocilizumab
Section titled “Tocilizumab”Intravenous tocilizumab has been reported to be effective for refractory OPN (literature reference only). 8)
8. References
Section titled “8. References”-
Leitão M, Davila Siliezar P, Laylani N, Lee AG. Myelin oligodendrocyte glycoprotein antibody disorder (MOGAD) optic perineuritis following severe COVID-19 infection. Am J Ophthalmol Case Rep. 2023;32:101952.
-
Ismail MA, Shariffudin NS, Bt Abd Jalil NF, Yew TC, Wan Hitam WH. Concurrent tuberculous optic neuritis and optic perineuritis in a patient with human immunodeficiency virus (HIV). Cureus. 2024;16(3):e55867.
-
Khan RR, Mahmood A, Kahlon S, Benyahia SA. Optic Perineuritis Secondary to CNS Involvement of Lymphoma. Cureus. 2024;16(12):e75818. doi:10.7759/cureus.75818. PMID:39822410; PMCID:PMC11735239.
-
Takada K, Fujiwara K, Ando E, et al. Optic perineuritis associated with nivolumab treatment for non-small cell lung cancer. Case Rep Oncol. 2021;14:792-796.
-
Droger SM, Hensen JH, van Rooij LC. Optic perineuritis in polyarthritis nodosa. BMJ Case Rep. 2021;14(7). doi:10.1136/bcr-2020-237988. PMID:34289998. PMCID:PMC8296769.
-
Tanaka Y, Nagatsuka H, Miki Y, et al. Two patients of visual disturbance and optic perineuritis after placement of a flow diverter. Radiol Case Rep. 2022;17:1487-1490.
-
Fatimah-Halwani I, Wahab Z, Masnon NA, et al. Bilateral optic perineuritis in tuberculosis-immune reconstitution inflammatory syndrome. Cureus. 2022;14(8):e27600.
-
Pickel L, Micieli JA. Spontaneous resolution of optic perineuritis in a patient with Crohn’s disease. Case Rep Ophthalmol. 2022;13:470-475.