Amiodarone is a diiodinated benzofuran derivative developed in the 1960s as an antianginal agent. It is classified as a class III antiarrhythmic drug but also possesses class I, II, and IV properties 1). It is widely prescribed for atrial fibrillation, ventricular tachycardia, and ventricular fibrillation, and is known in Japan by the brand name Ancaron (elsewhere as Cordarone, Pacerone, etc.).
Amiodarone has an oral bioavailability of 30–80% and an extremely long half-life of 20–100 days. It is highly lipophilic and accumulates in adipose tissue 1), and is metabolized by hepatic CYP3A4/CYP2C8 to produce the active metabolite desethylamiodarone (DEA) 1).
Vortex keratopathy (verticillate keratopathy): The most common ocular side effect. It appears as brown, whorl-like pigment deposits in the deep corneal epithelium and occurs in two-thirds of treated patients. It correlates with dose and duration, appearing in nearly 100% of patients on high doses (400 mg/day). It is graded using the Orlando classification (grade I–IV). Vortex keratopathy alone usually does not require discontinuation of amiodarone.
Others: Anterior subcapsular lens opacities, multiple chalazia, dry eye, etc.
Amiodarone also has various systemic side effects, including thyroid dysfunction, pulmonary toxicity (hypersensitivity pneumonitis, which can be fatal), peripheral neuropathy, and photosensitivity.
In a cohort study by Cheng et al. using the Taiwan National Health Insurance Database (6,175 patients in the amiodarone group vs. 24,700 controls), optic neuropathy was observed in 0.3% of the amiodarone group, with a hazard ratio of 2.09 (95% CI 1.13–3.85) compared to the non-treatment group (0.1%)1).
QWhat is the probability of developing optic neuropathy while taking amiodarone?
A
In a Taiwanese cohort study, optic neuropathy was observed in 0.3% of amiodarone users, with a hazard ratio of 2.09 compared to non-users1). Retrospective reports indicate an incidence of 0.36–2%, and the maximum estimated annual incidence in a prospective double-blind trial (over 1,600 patients) was 0.23–0.74%1).
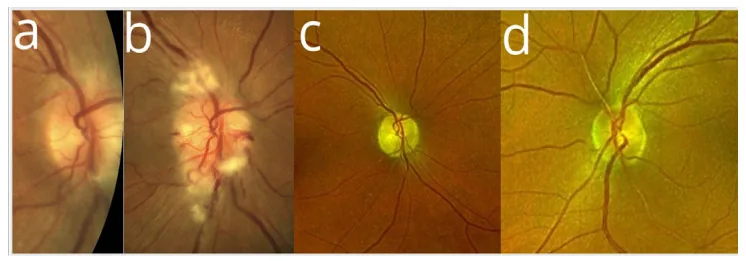
Dina Lešin Gaćina et al. Is Semaglutide Linked to NAION? A Case Report on a Rare Ocular Complication. Reports. 2025 Aug 20; 8(3):149. Figure 1. PMCID: PMC12372079. License: CC BY.
Decreased visual acuity: Acute or insidious onset. Can be monocular or binocular. In a review of 296 cases, 44% had insidious onset. The breakdown was: acute monocular 19%, insidious monocular 26%, acute binocular 10%, insidious binocular 14%.
Asymptomatic: Up to one-third of AAON patients have no subjective symptoms. It is often discovered only by optic disc edema.
Dyschromatopsia: Reported in some cases.
Clinical Findings (Findings Confirmed by Physician Examination)
The main clinical findings of AAON are shown below.
Optic disc edema: Present in 85% of cases, with two-thirds being bilateral and simultaneous. Optic disc edema persists for a median of 3 months (up to 15 months) after discontinuation of amiodarone.
Sequential optic disc swelling: A “sequential” pattern has been reported, where optic disc swelling appears in the contralateral eye 3 to 48 weeks after onset in one eye1).
Coexisting vortex keratopathy: Frequently observed in conjunction with optic neurotoxicity.
Patel et al. proposed the following five classifications2).
Insidious onset type
Most common classification: Presents with bilateral simultaneous papilledema and progresses slowly. Often has few subjective symptoms.
Non-arteritic anterior ischemic optic neuropathy-like type
Second most common classification: Presents with acute unilateral or bilateral vision loss, clinically very similar to non-arteritic anterior ischemic optic neuropathy.
Retrobulbar optic neuropathy type
Most difficult to diagnose: Presents with normal fundus, requiring imaging and blood tests for diagnosis.
Duration of amiodarone use: The average period until AAON onset is 9 months (range 1–84 months). Some reports indicate a median of about 4 months2). When the treatment duration exceeds a median of 41 days, the risk of optic neuropathy increases 3.5-fold1).
Cumulative dose: Cumulative dose and duration of administration are more important for risk assessment than daily dose1). The median dose in patients presenting with visual symptoms was 200 mg/day (range 57–1,200 mg/day).
Sex: In a review of 296 cases, the mean age was 66 years, and 74% were male. Men have approximately three times the risk of women1).
Hypertension: In men, amiodarone use and hypertension are significant risk factors for optic neuropathy1).
Coexisting cardiovascular risk factors: Many patients taking amiodarone have cardiovascular risk factors and are also at high risk for developing non-arteritic anterior ischemic optic neuropathy itself. Features of amiodarone-associated NA-AION include bilateral, insidious onset, generalized (non-altitudinal) visual field defects, and papilledema persisting for months.
QDoes reducing the dose of amiodarone decrease the risk of optic neuropathy?
A
Daily dose is not a significant risk factor; cumulative dose and duration of therapy are considered more important1). Reports indicate that the risk increases 3.5-fold when the median treatment duration exceeds 41 days, so follow-up is necessary even with short-term use.
All patients with NA-AION should be asked about amiodarone use, and if positive, the cardiology department should be notified. It is important to suspect drug-induced optic neuropathy by carefully reviewing medication history.
Differentiation from non-arteritic anterior ischemic optic neuropathy
Differentiating AAON from non-arteritic anterior ischemic optic neuropathy is the greatest clinical challenge. The main differentiating points are shown in the table below.
Care must also be taken to differentiate from giant cell arteritis. A case has been reported in which a 72-year-old man on amiodarone was suspected of having AAON, but giant cell arteritis was confirmed by temporal artery biopsy 3). In giant cell arteritis, biopsy can be positive even if ESR and CRP are normal 3). Additionally, in giant cell arteritis, MRI may show optic nerve sheath enhancement (optic perineuritis), a finding not reported in AAON 3).
Humphrey visual field test: Shows hemifield defects to central scotomas.
MRI: Usually normal in AAON; no optic nerve enhancement is seen. In suspected giant cell arteritis, check for optic nerve sheath enhancement (optic perineuritis) 3).
Visual outcomes after discontinuation are as follows:
Visual improvement: 58%
No change: 21%
Further visual decline: 21%
Legal blindness (20/200 or worse in at least one eye): 20%
No established drug therapy currently exists for AAON.
QWill vision recover if amiodarone is discontinued?
A
After discontinuing amiodarone, visual improvement occurs in only 58% of patients; 21% remain unchanged, 21% worsen further, and 20% progress to legal blindness (20/200 or worse). Additionally, because the half-life is long (20–100 days), the drug continues to remain in the body after discontinuation, which requires attention 1).
Accumulation of lamellar inclusions: Intracytoplasmic lamellar inclusions selectively accumulate in the cytoplasm of thick optic nerve axons. Similar changes are observed in the axons and Schwann cells of peripheral nerves in amiodarone-induced peripheral neuropathy.
Impaired axoplasmic flow: Lamellar bodies mechanically and biochemically reduce axoplasmic flow, which is considered the mechanism of optic nerve damage1). This disruption can cause papilledema.
Oxidative stress and apoptosis: Amiodarone induces mitochondrial H₂O₂ synthesis and reactive oxygen species (ROS) formation, leading to oxidative cell damage1).
Effects on retinal ganglion cells (RGCs): Rat experiments have confirmed RGCapoptosis and reduction in electroretinogram a-wave and b-wave amplitudes1).
QBy what mechanism does amiodarone damage the optic nerve?
A
Amiodarone inhibits lysosomal sphingomyelinase, inducing phospholipidosis, and lamellar inclusions accumulate in optic nerve axons1). This accumulation impairs axoplasmic flow, causing papilledema, and oxidative stress also contributes to cell damage, leading to reduced optic nerve function.
7. Latest Research and Future Perspectives (Investigational Reports)
Liao et al. (2007) showed in an RPE cell model that IGF-1 protects RPE cells from amiodarone-induced oxidative stress and apoptosis via the PI3K/Akt pathway1). RPE cell viability decreased in a concentration-dependent manner with amiodarone (LC50 = 50 μM), and IGF-1 suppressed this. Inhibition of the MAPK pathway did not affect the protective effect1).
A 2017 rat study showed that amiodarone affects the retinal ganglion cell layer, and IGF-1 reversed this effect1). The future application of IGF-1 in AAON treatment remains to be investigated.
In a prospective double-blind study by Mindel et al. (2007) involving over 1,600 participants with a median follow-up of 45.5 months, no cases of bilateral vision loss were reported, and the maximum estimated annual incidence was 0.23–0.74% 1). This contradicts previous retrospective reports (0.36–2%) and has led to ongoing debate about whether AAON is a distinct disease entity clinically different from non-arteritic anterior ischemic optic neuropathy.
Role of MRI in differentiating from giant cell arteritis
In cases of giant cell arteritis, MRI findings of optic perineuritis have been reported in 57–78% of cases, a finding not reported in AAON 3). Systematic evaluation of MRI findings in suspected AAON cases may contribute to improved diagnostic accuracy in the future.