Ethambutol (EMB) is a first-line drug used against Mycobacterium species, particularly Mycobacterium tuberculosis and nontuberculous mycobacteria such as Mycobacterium avium complex (MAC). The most serious side effect of EMB is ethambutol optic neuropathy (EON), which consistently ranks among the most frequent drug-induced optic neuropathies.
The prevalence of EON among patients receiving tuberculosis treatment is estimated at 1–2%. According to the World Health Organization (WHO), approximately 9.2 million new tuberculosis cases are reported annually, potentially resulting in up to 100,000 new cases of EON per year.
The risk of EON is highly dose-dependent. Estimated prevalence by EMB dose is shown below.
EMB dose
Estimated prevalence
<15 mg/kg/day
<1%
25 mg/kg/day
5–6%
>35 mg/kg/day
18–33%
However, EON has been reported even with low doses (<15 mg/kg). In a Japanese nationwide survey, 52.2% of EON cases occurred at low doses, indicating that there is no truly “safe” dose 3).
In 2009, the WHO revised its guidelines to include EMB in the continuation phase of tuberculosis treatment, extending the duration of administration. This change has raised concerns about an increased risk of developing EON 1).
QHow often does ethambutol optic neuropathy occur?
A
It occurs in about 1–2% of patients treated for tuberculosis. The risk increases with higher doses: 5–6% at 25 mg/kg/day and 18–33% at >35 mg/kg/day. It can also occur at low doses, so there is no truly safe dose. For details, see the section “What is Ethambutol Optic Neuropathy?“.
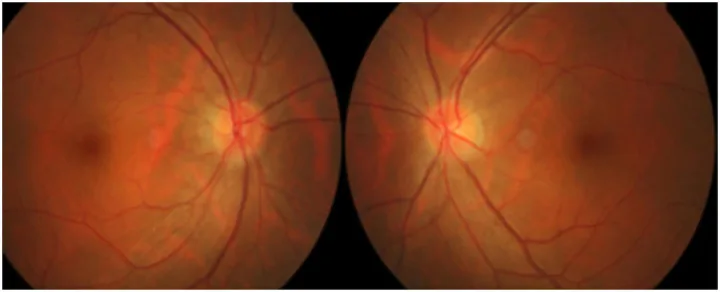
Sudhakar P, et al. Ethambutol optic neuropathy. Front Neurol. 2025. Figure 1. PMCID: PMC12460111. License: CC BY.
Image of a hyperemic optic disc in a patient with ethambutol optic neuropathy. This corresponds to disc hyperemia discussed in the section “2. Main Symptoms and Clinical Findings.”
Unlike other toxic optic neuropathies, EON can occur relatively soon after starting treatment. The onset ranges from 1 month to 36 months after starting medication, but it rarely occurs within 2 months, with an average of 7 months.
The main subjective symptoms are as follows:
Bilateral vision loss: Painless, symmetric, and insidious progression. Present in over 60% of patients.
Color vision abnormality: May be the first sign. Primarily red-green color deficiency, but blue-yellow abnormalities have also been reported. A complaint that red does not appear as bright as before can be a clue.
Blurred vision: The area of focus appears hazy.
Photophobia: Reported as a cone dysfunction due to ethambutol toxicity 5).
No eye movement pain: If pain is present, other diseases should be considered.
Clinical Findings (Findings Confirmed by Physician Examination)
Visual acuity: Ranges from mild (20/25) to severe (no light perception). Often mild in early stages.
Visual field: Central or paracentral scotoma (axial type) is most common. Sensitivity loss often begins temporally. Bitemporal hemianopia (extra-axial type) due to chiasmal involvement and peripheral visual field constriction can also occur.
Fundus findings: The optic disc appears normal initially (retrobulbar optic neuropathy). With progression, optic disc pallor, especially temporal pallor, appears. Disc pallor at onset suggests poor prognosis.
Critical flicker frequency: Decreased.
QWhat is the first symptom of ethambutol optic neuropathy?
A
Color vision abnormalities may be the first sign. A subjective feeling that red is not as vivid as before can be a clue. Since bilateral visual loss progresses insidiously, regular visual acuity and color vision checks are important for early detection.
The exact mechanism of EMB neurotoxicity is unknown, but metal chelation is considered the main cause. EMB and its metabolite 2,2-ethylenediaminodibutyric acid (EDBA) are both chelating agents and are thought to cause optic nerve damage through the following pathways 2).
Copper chelation: Chelates copper ions in mitochondrial cytochrome c oxidase, impairing oxidative phosphorylation.
Zinc chelation: Increases lysosomal membrane permeability and suppresses lysosomal activation.
Animal studies have shown that zinc deficiency is associated with myelin destruction and glial cell proliferation. In humans, long-term use of EMB may cause vitamin E and B1 deficiency, potentially worsening optic neuropathy.
Drug-induced optic neuropathies such as those caused by ethambutol, linezolid, and mesalamine are thought to result from acquired mitochondrial dysfunction, and their pathology is similar to hereditary Leber hereditary optic neuropathy.
High dose and long-term use: Risk increases depending on dose and duration of treatment.
Advanced age: Age 65 and older is high risk.
Renal impairment: EMB is excreted renally, and renal impairment leads to elevated blood levels.
Hypertension and diabetes: Underlying diseases affecting blood flow increase risk.
Smoking: It has been pointed out that smoking has an additive adverse effect on retinal ganglion cells.
Concomitant use of isoniazid: It is said to increase the incidence of toxic optic neuropathy.
Malnutrition: In developing countries, malnutrition increases risk and can lead to irreversible blindness1).
QWhich patients are at high risk for ethambutol optic neuropathy?
A
Risk factors include high dose and long-term use, age 65 years or older, renal dysfunction, hypertension, diabetes, smoking, and concomitant use of isoniazid. For details, see the “Causes and Risk Factors” section.
The diagnosis of EON is made clinically. Baseline examination before treatment is essential. It is recommended to perform visual acuity, visual field testing, critical flicker frequency, and color vision testing before starting EMB, and to check every 1 to 2 months during treatment.
Visual evoked potentials (VEP): Detect prolongation of P100 latency. It has been reported that P100 was prolonged to 107 ms or more in 34.8% of patients taking ethambutol2). Useful for detecting potential optic nerve damage, but not specific to EON.
OCT
Optical coherence tomography (OCT): Detect thinning of the peripapillary retinal nerve fiber layer (pRNFL) and changes in the ganglion cell layer-inner plexiform layer (GCIPL). Temporal-dominant changes are characteristic, with reductions of 20–79% reported2). Also useful for assessing visual prognosis.
Multifocal electroretinography (mfERG): Can detect potential retinal toxicity.
Electroretinography (ERG): Can detect cone dysfunction by delayed implicit time of flicker response5).
MRI: Necessary to rule out optic neuritis and other optic neuropathies. Usually normal in EON itself, but cases with T2 FLAIR hyperintensity of the optic chiasm have been reported2).
There is no established treatment for EON. No treatment is superior to discontinuation of the causative drug. When EON is suspected, prompt discontinuation of EMB is the most important action. Ophthalmologists should directly contact the prescribing physician before discontinuing EMB.
After discontinuation of EMB, visual acuity and visual field defects may continue to progress for about 2–3 months. Thereafter, gradual recovery occurs, but recovery is slow, taking from six months to two years.
Smoking should be discontinued as it has additive adverse effects in thinner abuse and EON. If underlying diseases affecting blood flow such as hypertension or diabetes are present, treatment should be coordinated with internal medicine.
In patients whose vision recovers, an average improvement of 2 lines on the Snellen chart is observed 2). However, some patients experience complete recovery of vision, while others have permanent visual impairment. The presence of optic disc pallor at onset is associated with a poor prognosis.
There are reports that RNFL thickness continues to decrease even after discontinuation of EMB, and irreversible vision loss can occur despite close monitoring and prompt drug discontinuation 2).
QWill vision recover if ethambutol is discontinued?
A
If EMB is discontinued before irreversible optic atrophy occurs, visual function improves in 30–64% of patients. However, complete recovery is rare, and the average improvement is 2 Snellen lines. Symptoms may continue to progress for 2–3 months after discontinuation, so continued follow-up is necessary. For details, see the section on Standard Treatment.
6. Pathophysiology and Detailed Mechanism of Onset
Both EMB and its metabolite EDBA act as metal chelators. EDBA has lower intraocular clearance than ethambutol itself, leading to higher local concentrations, and is estimated to contribute more to toxicity 2).
The main pathways of damage are as follows:
Mitochondrial damage: Chelation of copper ions in cytochrome c oxidase impairs oxidative phosphorylation 2).
Lysosomal damage: Chelation and accumulation of zinc increase lysosomal membrane permeability, leading to cell damage 2).
The parvocellular axons that make up the papillomacular bundle have particularly high mitochondrial energy demands. Therefore, in toxic and nutritional optic neuropathies, these axons are preferentially damaged 2).
It is presumed that among retinal ganglion cells, the p-cells, which consume large amounts of ATP, are predominantly affected, consistent with the formation of central scotomas. On the other hand, γ-cells involved in the pupillary light reflex are preserved, so the pupillary light reflex is relatively maintained.
Animal experiments suggest that axonal neuropathy caused by EMB tends to occur at the optic chiasm, which is consistent with the clinical presence of cases presenting with bitemporal hemianopia.
7. Latest research and future prospects (research-stage reports)
Sabhapandit et al. (2023) conducted a systematic review of 12 studies published between 2010 and 2021 (5818 individuals, 309 with EON) and reported that prolonged use of EMB beyond 2 months leads to significant optic nerve toxicity 1). Visual improvement after discontinuation of EMB was statistically significant (P = 0.035). Improvements in color vision abnormalities and visual field defects did not reach statistical significance.
Cases that can become irreversible even with low doses and short duration
Matsumoto et al. (2021) reported a case of an 85-year-old man who, despite low-dose EMB (12 mg/kg) and short duration (2.5 months), experienced rapid visual deterioration after discontinuation of EMB, leading to irreversible vision loss 3). Corrected visual acuity, which was 20/17 before discontinuation, dropped to 20/330 (right eye) and 20/1000 (left eye) within 3 weeks. This case demonstrates that even low doses can cause catastrophic vision loss.
Peterson & Hawy (2022) reported a case of late-onset EON in an 82-year-old man who had taken EMB at <15 mg/kg/day for 3 years during MAC treatment 4). Visual acuity improved after discontinuation of EMB, and the improvement persisted at 10 months. Although the median time to onset is reported as 9 months, this case shows that onset can occur even after more than 3 years.
Konana et al. (2024) reported three cases of cone dysfunction due to ethambutol toxicity 5). The main symptoms were photophobia and decreased visual acuity, and electroretinography showed delayed latency of flicker responses. This report suggests that ethambutol toxicity affects not only the optic nerve but also the retinal cell layers.
With the introduction of fixed-dose combination tablets (FDC: containing isoniazid, rifampicin, pyrazinamide, and ethambutol in one tablet) and the extension of treatment duration, an increase in the incidence of EON is anticipated 2). Important future research topics include establishing screening systems, verifying the usefulness of OCT and VEP in detecting subclinical EON, elucidating the pathogenesis of EON, and identifying risk factors.
Sabhapandit S, Gella V, Shireesha A, et al. Ethambutol optic neuropathy in the extended antitubercular therapy regime: A systematic review. Indian J Ophthalmol. 2023;71:729-735.
Sudhakar P, Acharya K, Kini TA. Ethambutol optic neuropathy. Frontiers in neurology. 2025;16:1626909. doi:10.3389/fneur.2025.1626909. PMID:41018187; PMCID:PMC12460111.
Matsumoto T, Kusabiraki R, Arisawa A, Fujiki T, Noda A, Tanaka A, et al. Drastically Progressive Ethambutol-induced Optic Neuropathy after Withdrawal of Ethambutol: A Case Report and Literature Review. Internal medicine (Tokyo, Japan). 2021;60(11):1785-1788. doi:10.2169/internalmedicine.6178-20. PMID:33390493; PMCID:PMC8222132.
Peterson E, Hawy E. Delayed and reversible ethambutol optic neuropathy. American journal of ophthalmology case reports. 2022;27:101611. doi:10.1016/j.ajoc.2022.101611. PMID:35756837; PMCID:PMC9218146.
Konana VK, Mooss V, Babu K. Cone dysfunction in patients with ethambutol toxicity. Indian journal of ophthalmology. 2024;72(7):1072-1074. doi:10.4103/IJO.IJO_494_23. PMID:38905470; PMCID:PMC11329819.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.