Nutritional Optic Neuropathy (NON) is a bilateral, symmetric, progressive optic nerve disorder caused by nutritional deficiencies. It belongs to the group of metabolic neuropathies and lies on the same spectrum as toxic optic neuropathy, but is distinguished by its nutritional cause.
The main causative nutrients are B vitamins (B12, B1, B2, B9) and copper. These are essential cofactors for mitochondrial oxidative phosphorylation.
Historically, outbreaks have been reported during famines and wars.
Strachan syndrome (1880s): Nutritional neuropathy prevalent among Jamaican sugarcane workers.
Tropical amblyopia: Reported in sub-Saharan Africa, including Nigeria.
Prisoner-of-war optic neuropathy: Occurred in Japanese prisoners during World War II.
Cuban epidemic optic neuropathy (1991–1993): The largest modern outbreak, affecting about 50,000 people.
Tanzanian epidemic optic neuropathy: Similar outbreaks have been reported.
In modern times, patients after bariatric surgery (BS) and those on restrictive or vegan diets are new risk groups. Neurological complications occur in about 4.6% of post-BS patients, including peripheral neuropathy (52%), Wernicke encephalopathy (9%), and night blindness (2.8%)2).
Onset in children has also been reported; in a literature review of 25 cases, 88% were boys and 68% had comorbid autism. Vitamin A and B12 deficiencies were the most common causes5).
QHow rare is nutritional optic neuropathy?
A
It is rare but easily overlooked. Historically, it occurred frequently during wars and famines. In modern times, new cases have been reported in patients after bariatric surgery and in those following a vegan diet, and the incidence is increasing.
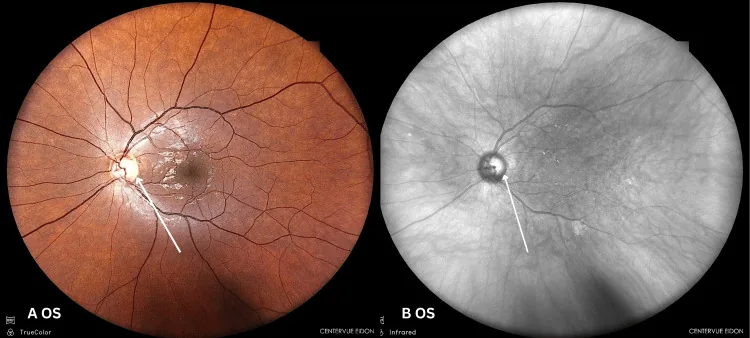
Nicolaou N, et al. Ethanol and Cyanide: A Case Report on Toxic and Nutritional Optic Neuropathy Associated With Alcohol and Tobacco. Cureus. 2025. Figure 4. PMCID: PMC12712447. License: CC BY.
Color fundus image and infrared fundus image of the left eye showing mild temporal pallor of the optic disc. This demonstrates a typical finding of optic neuropathy seen in nutritional optic neuropathy.
Visual loss: Subacute and progressive. Bilateral, symmetric, and painless.
Color vision deficiency (dyschromatopsia): Red-green color vision abnormalities appear early, presenting as complaints that red colors no longer appear as vivid as before.
Decreased contrast sensitivity: Difficulty distinguishing fine differences in brightness.
Central scotoma: Perceived as “blurring in the area of fixation.” Subsequently, it progresses to progressive visual loss.
Clinical Findings (Findings Confirmed by Physician Examination)
Pupillary light reflex: Often preserved. This is because the γ cells involved in the light reflex are spared.
Visual field: Central scotoma or centrocecal scotoma. Due to selective damage to the papillomacular bundle.
VEP: Reduced amplitude. Latency (P100) is normal or nearly normal.
OCT findings: Initially, RNFL (retinal nerve fiber layer) is normal. Thinning begins in the papillomacular bundle (temporal side) and extends to all quadrants. RNFL thinning is detected 3 months or more after onset 6). Meanwhile, GCL (ganglion cell layer) may show diffuse thinning preceding RNFL changes 1)4).
QIs it possible to have nutritional optic neuropathy even if OCT is normal?
A
Yes. Since RNFL thinning is detected 3 months or more after onset, visual dysfunction may occur even with normal OCT in the early stage 6). GCL analysis may detect abnormalities before RNFL changes 1)4), and VEP can sometimes detect functional visual pathway damage earlier.
Vitamin B12 (cobalamin): The most important cause of nutritional optic neuropathy. May be accompanied by pernicious anemia, subacute combined degeneration of the spinal cord, and peripheral neuropathy.
Vitamin B1 (thiamine): Involved in carbohydrate metabolism. Deficiency causes beriberi and Wernicke encephalopathy (impaired consciousness, memory disturbance, and oculomotor dysfunction).
Vitamin B6 (pyridoxine): Involved in the biosynthesis of neurotransmitters. The antituberculosis drug isoniazid antagonizes B6 metabolism and induces deficiency.
Vitamin B9 (folate): Coenzyme for purine and pyrimidine synthesis. Deficiency causes megaloblastic anemia and polyneuropathy predominantly with sensory disturbances.
Copper
Copper: Cofactor for oxidative phosphorylation and cellular metabolism. Leads to dysfunction of copper-dependent enzymes (oxidoreductases, monooxygenases).
It causes neuropathy in 10–20% of patients after gastric bypass surgery. Deficiency often develops more than 3 years after surgery, but onset at 18 months postoperatively has also been reported in cases with malnutrition 6).
Bariatric surgery: Roux-en-Y gastric bypass, biliopancreatic diversion, etc. Onset often occurs 1.5–3 years after surgery. Cases of onset at 7 months postoperatively have also been reported for B1, B6, and A deficiencies 2).
Strict vegan/vegetarian diet: High risk of B12, B1, and B9 deficiencies.
Pickiness/ARFID (Avoidant/Restrictive Food Intake Disorder): Important risk factor in children. After the COVID-19 pandemic, NON in normally developing children has increased 5).
Alcohol dependence: Not a direct cause, but frequently associated with B12 and B9 deficiencies.
Inflammatory bowel disease (IBD)/Celiac disease: Causes malabsorption of B12 and folate.
Pernicious anemia: B12 malabsorption due to intrinsic factor deficiency.
History of gastrointestinal surgery: Whipple procedure, colectomy, etc. 4).
Inappropriate parenteral nutrition: Risk of acute thiamine deficiency if vitamins are not supplemented.
QHow long after bariatric surgery does optic neuropathy typically develop?
A
Generally, onset occurs 1.5 to 3 years after surgery. Copper deficiency usually develops after more than 3 years, but cases with malnutrition have been reported as early as 18 months post-surgery6). When multiple nutrients are deficient, onset may occur earlier2).
Visual field test (HVF): To check for central scotoma or centrocecal scotoma.
VEP: Reduced amplitude, nearly normal latency. Can detect functional impairment even when OCT is normal6).
OCT (RNFL/GCL analysis): RNFL is normal in early stages. GCL analysis may detect abnormalities before RNFL changes, useful for early diagnosis and monitoring1)4).
Electroretinogram: Used to rule out retinal diseases.
MRI (brain/orbits): Essential to rule out compressive or demyelinating diseases.
Homocysteine, methylmalonic acid (MMA): Added when B12 is low or borderline. MMA rises only in B12 deficiency and is normal in folate deficiency, useful for differentiation.
Note that there are reports suggesting smoking is involved in the onset of LHON, and it is recognized to have similarities with NON in that both share a common mechanism of mitochondrial dysfunction leading to ATP deficiency.
Correction of the underlying nutrient deficiency is the cornerstone of treatment. A multidisciplinary approach (ophthalmology, gastroenterology, clinical psychology, nutrition, biochemistry) is recommended 6).
Oral administration (reversible causes): 1,000 μg/day for at least 1 month, then maintain the same dose. In mild deficiency, the dose may be reduced to 100–500 μg/day.
Intramuscular injection (irreversible causes, severe cases): 1,000 μg/day for 1 week → 1,000 μg/week for 1 month → maintenance dose of 1,000 μg/month indefinitely.
Routes of administration include oral, intranasal, sublingual, subcutaneous, and intramuscular.
For Wernicke encephalopathy, administer 100–1,000 mg. In cases of deficiency after bariatric surgery, there is a report of oral 100 mg three times daily for 3 days followed by 100 mg/day 2).
Use oral copper gluconate. In a report by Mosenia et al. (2024), 4 mg twice daily for 1 month was followed by a maintenance dose of 2 mg twice daily 4). In that report, serum copper levels normalized at 6 months, and visual acuity improved from hand motion to 20/25 OD and 20/40 OS after 2 years.
If the cause is removed early and vitamin supplementation is started, visual improvement can be expected. Recovery usually takes six months to two years. However, in chronic cases where optic atrophy has become established, recovery is limited to irreversible.
QCan vision recover with vitamin supplementation?
A
Good recovery can be expected with early detection and early treatment. In cases of copper deficiency, there are reports of significant visual recovery two years after starting supplementation4). On the other hand, in chronic cases with delayed diagnosis, visual recovery may be limited3). Starting treatment within three months is likely to lead to a good outcome.
B vitamins and copper are essential for mitochondrial oxidative phosphorylation involved in ATP production. Deficiencies in these nutrients block the electron transport chain, reducing ATP and accumulating free radicals (superoxide anions), leading to increased oxidative stress.
The selective vulnerability of the papillomacular bundle is attributed to the limited mitochondrial reserve of parvocellular RGCs (small-type retinal ganglion cells) that constitute this bundle, making them more prone to apoptosis4)6). The mechanism of tobacco-alcohol optic neuropathy is similar, with p-cells being preferentially damaged due to their high ATP consumption.
In toxic and nutritional optic neuropathies, the GCL (ganglion cell layer) has been shown to thin diffusely before the RNFL (retinal nerve fiber layer) in multiple case reports 1). RGC death involves mitochondrial dysfunction, caspase activation (especially caspase-7), and neurotrophin deficiency 1).
In hereditary optic neuropathy (ADOA), both the RNFL and GCL are affected simultaneously from the early stage, which contrasts with NON 1).
Sriram et al. (2021) reported that in five cases of toxic and nutritional optic neuropathy, the RNFL was relatively preserved while the GCL showed diffuse thinning 1). Ethambutol has also been shown to exert excitotoxicity on RGCs, selectively damaging the RGC layer via endogenous glutamate.
Vitamin B9 and B12 deficiency: These vitamins act as cofactors in reactions that use formate for purine synthesis. Deficiency leads to formate accumulation, which inhibits the electron transport chain, suppressing mitochondrial function and leading to ATP depletion 3). Additionally, B12 is a cofactor for myelin synthesis; its deficiency causes demyelination and axonal damage in the optic nerve. In heavy alcohol drinkers, the direct neurotoxicity of alcohol combined with B1 and B12 deficiency amplifies the damage.
Copper deficiency: It causes dysfunction of copper-dependent enzymes (oxidoreductases, monooxygenases). This results in combined impairment of neurotransmitter conversion, oxidative phosphorylation, and free radical removal.
7. Latest Research and Future Perspectives (Research-stage Reports)
Multiple case reports have confirmed that GCL can become thin early even when RNFL is normal1)4). Data from the glaucoma field suggest that GCL analysis may be more sensitive than RNFL in early stages4). It is expected that GCL analysis will be routinely incorporated into severity assessment and follow-up monitoring of NON in the future.
Teng et al. (2025) reported three developmentally normal children (13–15-year-old boys) with NON primarily due to B12 deficiency caused by selective eating (including ARFID)5). A literature review indicated that among 25 pediatric NON cases, 68% had autism and 88% were boys, highlighting the importance of recognizing risk factors other than autism (traumatic eating experiences, multiple food allergies, ARFID).
Eating disorders in children have increased after the COVID-19 pandemic, and reports of NON in developmentally normal children are gaining attention as a new challenge.
Importance of Early Treatment in Copper Deficiency Optic Neuropathy
Mosenia et al. (2024) reported a case of copper deficiency optic neuropathy after gastrointestinal surgery, where copper gluconate supplementation improved visual acuity from counting fingers (CF) to 20/25 OD and 20/40 OS after two years4). Notably, GCL thinning was detected even when RNFL was normal.
Since recovery is limited in long-term untreated cases, regular copper monitoring for patients after gastrointestinal surgery is recommended.
Zainuddin et al. (2025) reported a case of copper deficiency NON after gastric bypass, where gastric bypass reversal to normal anatomy, along with TPN, copper supplementation, and multivitamins, improved visual acuity to 6/6 and N56). However, central scotoma persisted after 18 months.
Reversal surgery is gaining attention as an option to fundamentally resolve malabsorption, but patient selection criteria and long-term outcomes require further study.
Sriram A, Miao Y, Subramanian P, Schultz JS, Zhang C. A differential loss of nerve fiber layer thickness and retinal ganglion cell complex in toxic and nutritional optic neuropathy. Adv Ophthalmol Pract Res. 2021;1:100026.
Khalid MJ, Ayub MA, Kataria S, Hebert M, Parvathaneni A. Concomitant occurrence of peripheral neuropathy and vision loss due to multivitamin deficiency after bariatric surgery. Cureus. 2024;16(5):e59959.
Othman I, Tai E, Kuganasan S, Abu N. Vision Loss as a Presenting Symptom of Vitamin B12 Deficiency. Cureus. 2024;16(5):e60113. doi:10.7759/cureus.60113. PMID:38864050; PMCID:PMC11164691.
Mosenia A, Khan S, Aung MH. Visual recovery in a patient with optic neuropathy secondary to copper deficiency. Am J Ophthalmol Case Rep. 2024;36:102197.
Teng RW, Heidary G, Gise RA. Selective diet induced nutritional optic neuropathy in developmentally normal children. Am J Ophthalmol Case Rep. 2025;37:102234.