Dysthyroid optic neuropathy (DON) is an optic nerve dysfunction associated with thyroid eye disease (TED). TED, also known as Graves orbitopathy (GO), is an autoimmune disease in which enlargement of the extraocular muscles and orbital fat increases intraorbital pressure, compressing the optic nerve. It is one of the most severe complications of TED and, if left untreated, can lead to permanent vision loss.
DON occurs in 0.9–8.6% of all TED cases1), and approximately 70% of cases are bilateral. More than half of patients maintain a corrected visual acuity of 0.5 or better, but in the worst cases, it can lead to blindness. Since visual function can be expected to recover with appropriate treatment, early diagnosis is extremely important.
QIf I have thyroid eye disease, will I definitely develop DON?
A
Only about 3–8% of all TED cases develop DON, so the majority of TED patients do not progress to DON. However, caution is needed if there are risk factors such as the myopathic phenotype, smoking, or older age. For details, see the section on Causes and Risk Factors.
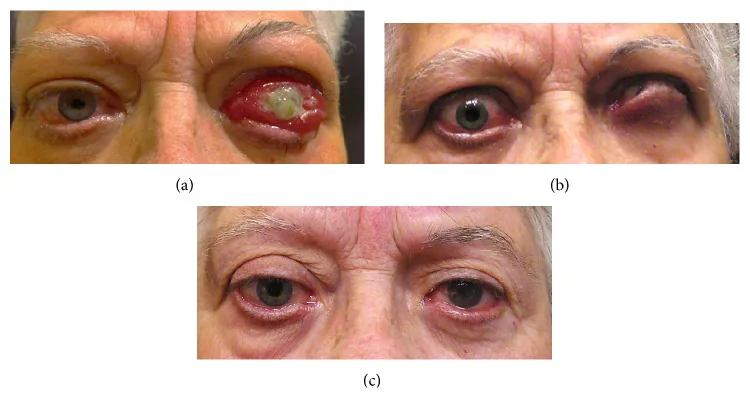
Jesús Barrio-Barrio, Alfonso L Sabater, Elvira Bonet-Farriol et al. Graves’ Ophthalmopathy: VISA versus EUGOGO Classification, Assessment, and Management. Journal of Ophthalmology. 2015 Aug 17; 2015:249125. Figure 4. PMCID: PMC4553342. License: CC BY.
The initial symptoms of DON are blurred central vision and decreased color vividness (desaturation). The degree of visual loss varies from mild to no light perception, but more than half of patients maintain visual acuity of 0.5 or better.
The main subjective symptoms are listed below.
Visual loss: Perceived as foggy central vision. It follows an acute to subacute course.
Desaturation: Colors, especially red, appear less vivid than before.
Diplopia: In the myomatous phenotype, diplopia is often reported due to restricted eye movement.
Orbital discomfort: A dull, aching pain may be felt.
Congestive soft tissue signs: Eyelid swelling, conjunctival injection and edema become prominent.
Elevated intraocular pressure on upgaze: An increase of more than 9 mmHg may be observed.
Proptosis: Not necessarily prominent in DON. It is thought that tight eyelids restrict forward movement of the globe, leading to diffuse elevation of orbital pressure.
76% of DON cases are bilateral, and optic disc swelling is absent in about half. Since DON can occur even without optic disc abnormalities, a combination of visual function tests and imaging is essential.
TED is an autoimmune disease caused by autoantibodies against TSH receptors and IGF-1 receptors on the surface of orbital fibroblasts. Antibody binding leads to adipogenesis, T lymphocyte activation, and cytokine release, resulting in deposition of glycosaminoglycans (GAGs) in orbital fat and muscles.
TED is broadly divided into two phenotypes.
Adipogenic Type
Also known as: Type I, adipogenic type
Features: Mainly presents with fat expansion and scarring of the levator palpebrae superioris muscle. Accounts for about two-thirds of TED patients.
Association with DON: Rarely leads to DON unless severe proptosis causes optic nerve stretching.
Myopathic Type
Also known as: Type II, myopathic type
Features: Involves hypertrophy of extraocular muscles, presenting with congestive soft tissue signs and ocular motility disorders. Accounts for about one-third of TED patients.
Association with DON: Prone to optic nerve compression at the orbital apex, a major cause of DON.
TED itself is more common in women (female-to-male ratio 4:1), while DON tends to occur in older men. Major risk factors are listed below.
Smoking: The greatest risk factor for TED progression and DON development.
Advanced age: Severe TED is more frequent in people aged 60 and older.
Diabetes: As a comorbid condition, increases the risk of DON.
Radioactive iodine therapy (RAI): Increases the risk of TED progression by up to 40%.
Immune response stimulators: Include intermittent infections, local surgery, and other triggering factors.
Thyroid dysfunction correlates with the severity of TED, but there is no clear correlation with the onset or severity of DON. Additionally, DON can occur even if all thyroid autoantibodies are negative.
QHow much does smoking increase the risk of DON?
A
Smoking is considered the most important risk factor for the progression of TED and the development of DON. The risk of worsening TED after radioactive iodine therapy is also higher in smokers. It is known that smoking cessation reduces treatment resistance in TED.
Automated perimetry: The most commonly performed test. Central and paracentral scotomas are common. Inferior arcuate scotomas, horizontal defects, generalized sensitivity loss, and enlarged blind spots are detected in about 70% of cases.
Color vision test: In asymmetric optic neuropathy, it is detected as reduced color saturation in the more affected eye. In symmetric and slowly developing cases, it may not be apparent.
RAPD test: A simple and useful method for detecting optic neuropathy. It is negative in symmetric involvement.
Flicker test: Useful as an early indicator of decreased optic nerve function.
VEP (Visual Evoked Potentials): About three-quarters of DON cases show prolonged latency and reduced amplitude. It is used as an adjunct when clinical findings or visual field results are ambiguous.
OCT (Optical Coherence Tomography): Can objectively evaluate thinning of the retinal nerve fiber layer (RNFL) and macular ganglion cell complex (GCL).
Imaging is essential for definitive diagnosis and surgical planning of DON.
Test
Main Advantages
CT
Excellent bone visualization. Ideal for surgical planning.
MRI (STIR)
Useful for assessing inflammatory activity.
CT: Frequently detects apical crowding at the orbital apex. Severe apical crowding is a predictor with 62% sensitivity and 91% specificity. When apical disappearance of the optic nerve exceeds 50%, sensitivity is 80% and specificity 70.6%. Also used for surgical planning and intraoperative navigation.
MRI: Inflammatory activity can be assessed especially with STIR (short tau inversion recovery) sequences. Hypertrophy of the medial rectus and superior rectus-levator complex increases the incidence of DON. Since coronal sections alone may miss optic nerve compression near the annulus of Zinn, combined use of axial imaging is important.
Reports indicate that 96% of patients with recent DON have high titers of thyroid-stimulating immunoglobulin (TSI). However, DON can occur even when all autoantibodies are negative, so serological tests alone cannot rule out the diagnosis.
QWhich should be prioritized, CT or MRI?
A
CT is often the first choice because it provides excellent bone visualization, is quick and inexpensive, and is suitable for surgical planning. On the other hand, MRI STIR sequences are superior for assessing inflammatory activity. The two are complementary and should be used according to the situation.
The first-line treatment for DON is steroid pulse therapy (or half-pulse therapy).
Steroid pulse therapy: Methylprednisolone (IVMP) 1 g/day intravenously for 3 consecutive days. This is considered one course, and 1 to 3 courses are administered1).
Maintenance therapy: After pulse therapy, switch to oral prednisolone. Rapid tapering should be avoided as it may cause recurrence of optic neuropathy.
Cumulative dose limit: If the cumulative dose exceeds 8 g in prednisolone equivalent, the risk of death due to acute liver injury increases1). Japanese guidelines recommend pre-treatment tests such as liver function tests, hepatitis virus tests, and T-SPOT tests before pulse therapy1).
The EUGOGO guidelines (2021) recommend high-dose administration of up to 1 g per day for 3 days, repeated weekly if improvement is seen.
External beam radiotherapy (EBRT) targets lymphocytes and fibroblasts to suppress inflammation. It is not used alone as acute treatment due to lack of rapid effect, and is positioned as an adjunct to steroid therapy. Combined with steroids, it has been reported to prevent the onset of DON.
If optic nerve function does not improve within 2 weeks after starting steroid pulse therapy, emergency orbital decompression surgery is considered. In Japan, 22–38% of DON patients undergo orbital decompression surgery1).
Surgical approaches include the following:
Transcutaneous approach: Reaches the deep lateral wall through an upper eyelid crease incision.
Transconjunctival approach: Reaches the orbital floor including the medial wall and posterior strut.
Transnasal endoscopic approach: Used for approach via the medial wall.
Decompression of the optic nerve is achieved by expanding the volume at the orbital apex, targeting the medial wall, orbital floor, and deep lateral wall. Preoperative CT planning and intraoperative navigation are useful.
Radioactive iodine (RAI) treatment may worsen symptoms in up to 20% of existing TED patients. Prophylactic administration of oral prednisone before RAI is recommended. Factors associated with worsening of TED after RAI include smoking, high pre-treatment T3 levels, post-treatment hypothyroidism, and large goiter.
With appropriate treatment, visual function recovery is achieved in approximately 70% or more of patients. The probability of complete visual recovery is higher when surgical decompression is performed.
QWhat happens if there is no improvement with steroid pulse therapy?
A
If no improvement in optic nerve function is seen within two weeks after starting pulse therapy, emergency orbital decompression is considered. In Japan, 22–38% of DON patients undergo orbital decompression1).
Multiple mechanisms are involved in the development of DON.
Compressive mechanism (most important): Enlarged extraocular muscles compress the optic nerve at the orbital apex, impairing axoplasmic flow. The fact that visual acuity and visual field recovery can be obtained immediately after orbital decompression strongly supports this mechanism. The medial rectus and superior rectus/levator complex are close to the optic nerve when passing through the annulus of Zinn, so hypertrophy of these muscles particularly increases the incidence of DON.
Stretching mechanism (rare): Severe proptosis stretches the optic nerve, impairing axonal function and blood flow. This is much rarer than the compressive mechanism.
Inflammatory mechanism: Inflammation within the orbit causes optic neuritis. The effectiveness of corticosteroids supports this mechanism.
As the underlying pathology of TED, autoantibodies bind to TSH receptors and IGF-1 receptors on orbital fibroblasts with multipotent capacity, leading to the following cascade.
Fibroblasts differentiate into adipocytes or myofibroblasts
Activation of T lymphocytes produces inflammatory cytokines such as TNF-α and IL-6
Deposition of glycosaminoglycans (GAG) and hyaluronic acid leads to orbital edema and muscle enlargement
As a result of these processes, the volume within the orbit increases, causing compression or stretching of the optic nerve under the constraints of the bony orbit.
7. Latest Research and Future Perspectives (Investigational Reports)
Teprotumumab is a monoclonal antibody that specifically binds to the extracellular domain of the IGF-1 receptor (IGF-1R) and inhibits the immune response in TED.
Cong et al. (2024) reported in a meta-analysis of 5 RCTs (total 411 cases) that teprotumumab significantly reduced proptosis, improved clinical activity score (CAS), and improved diplopia compared to placebo. The risk of adverse events and serious adverse events was not significantly different from the placebo group 2).
For DON, multiple observational studies have reported that teprotumumab was effective in cases resistant to steroids, radiation therapy, and surgery. Future research is expected on the efficacy of teprotumumab in Japanese patients 1).
Mizuochi et al. (2025) reported a case of a 55-year-old woman who transitioned from hypothyroidism to Graves’ disease and developed DON. After three courses of 1 g pulse therapy, she progressed to DON, but additional pulse therapy restored her vision. However, disease activity persisted for more than four years, with a total of five exacerbations. She underwent repeated outpatient 0.5 g once-weekly pulse therapy, and the cumulative dose of methylprednisolone reached 59.5 g, but no serious adverse effects were observed 1).
This report suggests the importance of careful monitoring (CAS, TSAb, orbital MRI) in the long-term management of DON.
QCan teprotumumab be used for DON?
A
Currently, teprotumumab is not established as a standard treatment for DON. However, several observational studies have reported its efficacy in DON cases resistant to steroids or radiation therapy, and future research is expected.
Mizuochi K, Hiromatsu Y, Nakamura Y, et al. Transition from hypothyroidism to Graves’ disease, development of thyroid eye disease, progression to optic neuropathy after inpatient pulse therapy, and long-term administration of outpatient pulse therapy: a case report with review of literature. Endocr J. 2025;72(1):115-122.
Cong X, Pei L, Hu H. Teprotumumab for treating active thyroid eye disease: A meta-analysis. Medicine. 2025;104(26):e42966. doi:10.1097/MD.0000000000042966. PMID:40587732; PMCID:PMC12212777.