Neuromyelitis optica spectrum disorder (NMOSD) is an inflammatory, antibody-mediated, autoimmune disease of the central nervous system. Formerly called Devic’s disease, it was long considered a subtype of multiple sclerosis (MS). However, the discovery of autoantibodies against aquaporin-4 (AQP4-IgG) in 2004 established it as a distinct disease entity.
Historical background: In 1870, Sir Thomas Clifford Allbutt first described the association between myelitis and optic nerve involvement. Subsequent research recognized it as a disease distinct from MS, and it is now understood under the comprehensive concept of NMOSD.
Epidemiology is as follows:
Incidence: The estimated annual incidence of AQP4+ NMOSD is 0.4–7.3 per million people1)
Sex ratio: The female-to-male ratio is approximately 9:1, with a marked female predominance.
Age of onset: Mainly occurs in middle age (40–60 years), with a peak in the late 30s to early 40s.
Race: More common in people of African and Asian descent1)
Association with pregnancy: About 20–47% of women experience their first attack during pregnancy or within one year after childbirth or miscarriage.
QHow is NMOSD different from multiple sclerosis (MS)?
A
NMOSD is an antibody-mediated disease targeting the AQP4 water channel on astrocytes, and its pathology, treatment, and prognosis are fundamentally different from MS. In NMOSD, longitudinally extensive transverse myelitis (LETM) and severe optic neuritis are typical, and an important difference is that disease-modifying drugs effective for MS, such as interferon beta, may trigger relapses in NMOSD.
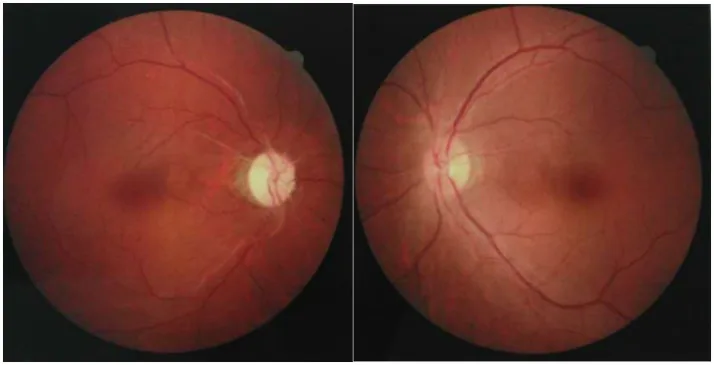
Chuai Y, et al. Paraneoplastic neuromyelitis optica spectrum disorder with dual AQP4-IgG and CRMP5 antibodies following thymectomy: a case report. Front Neurosci. 2026. Figure 1. PMCID: PMC13006573. License: CC BY.
Fundus photographs of both eyes showing optic atrophy due to pallor of the optic disc in one eye and mild optic disc swelling in the other eye. These findings represent the acute to chronic phase of optic neuritis seen in NMOSD.
Symptoms of NMOSD vary depending on the affected site.
Rapid vision loss: One of the main symptoms. It is characteristically resistant to steroid therapy.
Eye pain: Associated with optic neuritis, occurring in about half of cases.
Color vision abnormalities: Typically a decrease in red saturation.
Visual field defects: Not limited to central scotoma; may also cause horizontal hemianopia, bitemporal hemianopia, or homonymous hemianopia because lesions can extend to the optic chiasm and optic tract.
Sensory disturbances and paraplegia: Motor and sensory deficits due to myelitis.
Bladder and rectal dysfunction: Autonomic neuropathy associated with myelitis
Intractable hiccups, nausea, and vomiting: Characteristic symptoms due to area postrema lesions
Oculomotor disturbance: Due to brainstem lesions
Hypersomnia (narcolepsy-like): Due to diencephalic/hypothalamic lesions
In the early stages, influenza-like symptoms (fever, myalgia, headache) may occur.
Bilateral simultaneous onset: Optic neuritis in NMOSD is bilateral in 17–82% of cases. An important distinction from MS.
Severe visual loss: In AQP4+ NMOSD, the median nadir visual acuity is hand motion (HM) level. Even after recovery, the median visual acuity is counting fingers, and 60–69% of patients have permanent visual impairment of 20/200 or worse in at least one eye.
Myelitis
LETM (Longitudinally Extensive Transverse Myelitis): Continuous lesions spanning three or more vertebral segments. Seen in approximately 85% of AQP4+ NMOSD patients during acute myelitis.
Complete spinal cord syndrome: Involvement of all three pathways: motor, sensory, and autonomic.
Severe functional impairment: More than 30% of patients are wheelchair-dependent at the nadir of an attack. 37–44% of AQP4+ NMOSD patients eventually require walking aids.
Area Postrema Syndrome
Intractable hiccups: Persisting for days to weeks, unresponsive to conventional antiemetics.
Nausea and vomiting: Because the area postrema lacks a blood-brain barrier, it is a site where AQP4-IgG can easily reach directly.
Core diagnostic finding of NMOSD: Unexplained intractable hiccups should raise strong suspicion of NMOSD.
QHow does optic neuritis in NMOSD differ from that in MS?
A
Optic neuritis in NMOSD is more severe, bilateral, and recurrent, with a poor visual prognosis. In AQP4+ NMOSD, 60–69% of patients are reported to have permanent visual impairment of 20/200 or worse in at least one eye. Additionally, it frequently involves the optic chiasm, causing various visual field defects such as bitemporal hemianopia, which also distinguishes it from MS.
Spinal cord MRI: LETM is most characteristic. Central gray matter predominance. Associated with spinal cord swelling, T1 hypointensity, and Gd enhancement. Approximately 85% of AQP4+ NMOSD present with LETM during acute myelitis 1)
Optic nerve MRI: Fat-suppressed imaging is essential. Bilateral, long-segment inflammation (≥50%) is characteristic. Involvement of the posterior portion and optic chiasm is typical of AQP4+ NMOSD 1)
Brain MRI: Area postrema lesions, periependymal brainstem lesions around the fourth ventricle, hypothalamic/third ventricle periventricular lesions, and extensive white matter lesions may be observed
Characteristics of NMOSD: Unlike MS, asymptomatic new T2 lesions are rare (3–13%). Surveillance MRI is usually not required 1)
In elderly patients, differentiation from ischemic optic neuropathy, cervical spondylotic myelopathy, spinal cord infarction, and primary CNS lymphoma is important
QCan NMOSD be diagnosed even if AQP4 antibody is negative?
A
Yes. Even if AQP4-IgG is negative or untested, NMOSD can be diagnosed if two or more core clinical characteristics are met, additional MRI requirements are fulfilled, and other diseases are excluded. Additionally, approximately 30% of AQP4-IgG-negative cases are positive for MOG-IgG, and testing for both antibodies is recommended. Less than 1% of AQP4-IgG-negative cases later seroconvert.
Methylprednisolone 1,000 mg/day intravenous infusion for 3 days
If no improvement in vision, consider another course after an interval of 3–4 days
Optic neuritis in NMOSD is highly resistant to steroids; if response is insufficient, consider next treatment early
Second-line: Plasma exchange therapy
Performed when there is no response to steroid pulse. The following methods are options.
Simple plasma exchange (PE): Most effective but also causes the greatest damage to the body
Double filtration plasmapheresis (DFPP)
Immunoadsorption therapy (IA): Allows selective removal of antibodies
The order of effectiveness is simple plasma exchange > double filtration > immunoadsorption. One course consists of 5–6 sessions, and hospitalization is required until recovery of total IgG levels after treatment. Note that for “optic neuritis,” it may not be covered by insurance, and explanation to the patient is necessary.
In AQP4+ NMOSD, maintenance treatment should be started early after the first attack 1). After plasma exchange, transition to prednisolone 5–10 mg/day plus azathioprine 50–100 mg/day is common.
Biologics with high levels of evidence are as follows.
Complement inhibitors
Eculizumab: 900 mg IV weekly × 4, then 1,200 mg every 2 weeks for maintenance 1)
Ravulizumab: Weight-based loading dose (2,400–3,000 mg) → 3,000–3,600 mg every 8 weeks starting from day 151)
B-cell depletion therapy
Rituximab: 375 mg/m² IV weekly × 4, or 1,000 mg × 2 (2 weeks apart) → 1,000 mg × 2 every 6 months1)
Inebilizumab: 300 mg IV twice, 15 days apart → every 6 months1)
IL-6 receptor inhibitor
Satralizumab: 120 mg subcutaneous injection every 4 weeks1)
QWhat if steroid pulse therapy is ineffective?
A
Plasma exchange therapy is the next option. Choose from simple plasma exchange, double filtration plasmapheresis, or immunoadsorption. Simple plasma exchange is considered most effective but also places a greater burden on the body. One course consists of 5–6 sessions, and hospitalization is required after treatment.
NMOSD is essentially an astrocytopathy. The pathogenesis is as follows.
Antibody production and blood-brain barrier (BBB) crossing
In the periphery, B cells differentiate into AQP4-IgG-secreting plasmablasts. IL-6 promotes this differentiation and enhances blood-brain barrier permeability. The area postrema lacks a blood-brain barrier and can serve as a route for AQP4-IgG entry into the CNS.
Cascade of astrocyte damage
AQP4-IgG binds to AQP4 water channels highly expressed on astrocyte end-feet, leading to astrocyte injury through the following pathways:
Classical complement pathway activation: The Fc portion of AQP4-IgG activates complement, forming the membrane attack complex (MAC) and directly damaging astrocytes.
Antibody-dependent cell-mediated cytotoxicity (ADCC): NK cells and neutrophils damage astrocytes via Fcγ receptors.
In MS, CD8+ T cells play a central role with predominant white matter demyelination, whereas in NMOSD, CD4+ T cells are more involved, forming necrotic lesions affecting both gray and white matter.
Reason for distribution
AQP4 channels are abundantly distributed in the optic nerve, area postrema, and spinal cord, making these regions selectively targeted.
Biomarkers
Serum GFAP: Reflects astrocyte damage and is elevated during attacks.
Serum neurofilament light chain (NfL): Reflects axonal damage and correlates with attack severity1).
Cytokines involved include IL-6, IL-10, IL-17a, G-CSF, TNF-α, and BAFF/APRIL.
7. Latest Research and Future Prospects (Investigational Reports)
It is estimated that 3–5% of NMOSD cases are paraneoplastic. Cases associated with ovarian teratoma have been studied in particular detail.
Ikeguchi et al. (2021) conducted a review of 6 cases of ovarian teratoma-associated AQP4+ NMOSD 2). All patients were female, with a mean age at onset of 32.7 years (range 15–50). Among the 6 cases, 83% (5/6) presented with nausea and vomiting, 83% had positive CSF oligoclonal bands, and 83% had dorsal brainstem lesions. Pathological analysis confirmed AQP4 immunoreactivity and lymphocyte infiltration in GFAP-positive neural tissue within the tumor, suggesting that AQP4 antigen presentation within the tumor triggers an autoimmune response. After tumor resection, AQP4-IgG seroconverted to negative in 60% (3/5) of cases.
Ding et al. (2021) conducted a review of 43 cases of paraneoplastic NMOSD 3). 88.4% were female, with breast cancer and lung cancer being the most common tumor types. The importance of tumor screening is emphasized, especially in NMOSD patients aged 50 years or older.
Screening for tumors, including teratomas, is recommended even in young patients.
The efficacy of Protein-A immunoadsorption (IA) has been reported for refractory NMOSD unresponsive to steroids, plasma exchange, and rituximab.
Fan et al. (2024) performed three sessions of Protein-A immunoadsorption in a 35-year-old woman with refractory NMOSD complicated by Sjögren’s syndrome that did not respond to steroid pulse therapy and IVIG4). Within one week, visual impairment, paraplegia, and proprioceptive sensory deficits markedly improved, and rapid decreases in AQP4-IgG, IgA, IgG, and IgM were confirmed. No relapse or progression was observed during 4 years of follow-up.
Characteristics of Cases with Concurrent Autoimmune Diseases
The actual status of various autoimmune diseases complicating NMOSD is becoming clearer.
Zhu et al. (2025) reported the case of a 14-year-old girl who developed NMOSD at age 11 5). She was AQP4-IgG positive, and primary Sjögren’s syndrome was confirmed during the course. Remission was maintained with methylprednisolone, IVIG, and a switch from mycophenolate mofetil (MMF) to tacrolimus. Although 20–30% of adult NMOSD cases have been reported to have concurrent autoimmune diseases, this case demonstrates that such comorbidity can also occur in pediatric patients 5).
Cacciaguerra L, Flanagan EP. Updates in NMOSD and MOGAD Diagnosis and Treatment. Neurol Clin. 2024;42(1):77-114.
Ikeguchi R, Shimizu Y, Shimomura A, Suzuki M, Shimoji K, Motohashi T, Yamamoto T, Shibata N, Kitagawa K. Paraneoplastic AQP4-IgG-Seropositive Neuromyelitis Optica Spectrum Disorder Associated With Teratoma: A Case Report and Literature Review. Neurol Neuroimmunol Neuroinflamm. 2021;8(5):e1045. doi:10.1212/NXI.0000000000001045. PMID: 34285095. PMCID: PMC8293286.
Ding M, Lang Y, Cui L. AQP4-IgG positive paraneoplastic NMOSD: A case report and review. Brain and behavior. 2021;11(10):e2282. doi:10.1002/brb3.2282. PMID:34520629; PMCID:PMC8553315.
Fan W, Chen X, Xiao P, Wei B, Zhang Y, Huang J, et al. Protein-A immunoadsorption combined with immunosuppressive treatment in refractory primary Sjögren’s syndrome coexisting with NMOSD: a case report and literature review. Frontiers in immunology. 2024;15:1429405. doi:10.3389/fimmu.2024.1429405. PMID:39055718; PMCID:PMC11269126.
Zhu G-q, Hu R-x, Peng Y, et al. A Chinese girl with neuromyelitis optica spectrum disorder coexisting with primary Sjogren’s syndrome: a case report and literature review. Front Immunol. 2025;16:1559825.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.