Penetrating Eye Injury
Definition: Entrance wound only (no exit wound)
Anterior prolapse of intraocular contents occurs only at the entry site. Relatively less severe than perforating injuries.

A penetrating eye injury is an open globe injury caused by a sharp object, with only an entrance wound and no exit wound. According to the Birmingham Eye Trauma Terminology, it is defined as “penetrating if there is an entrance wound but no exit wound”; even if there are multiple lacerations, they are classified as penetrating if they result from multiple entry mechanisms.
Cases involving an intraocular foreign body (IOFB) are classified separately. Injuries with both entrance and exit wounds are distinguished as perforating eye injuries.
Penetrating Eye Injury
Definition: Entrance wound only (no exit wound)
Anterior prolapse of intraocular contents occurs only at the entry site. Relatively less severe than perforating injuries.
Perforating Eye Injury
Definition: Entrance wound + exit wound
Because the globe is completely penetrated, intraocular contents prolapse from both front and back, making it more severe.
Intraocular Foreign Body (IOFB)
Definition: Retention of a foreign body inside the eyeball
May be associated with penetrating trauma. CT examination should be performed as needed.
The location of injury affects prognosis and is classified into the following three zones1).
| Zone | Extent | Characteristics |
|---|---|---|
| Zone I | Cornea to limbus | Limited to the anterior segment. Relatively good prognosis |
| Zone II | Up to 5 mm posterior to the limbus | Anterior to the ora serrata. Frequent damage to the lens and iris |
| Zone III | More than 5 mm posterior to the limbus | Posterior segment including the retina. Often poor prognosis |
| Item | Penetrating | Perforating |
|---|---|---|
| Entry wound | Present | Present |
| Exit wound | Absent | Present |
| Ocular content prolapse | Only at entry (anterior) | Both anterior and posterior |
| Severity | Relatively mild | Relatively severe |
| IOFB present | May be present | Rare (falls out after perforation) |
The incidence of open globe injury is estimated at approximately 3.5–4.5 per 100,000 population 1). The majority of patients are male, with a relative risk about 5.5 times higher than females. The average age at injury is about 30 years. A systematic review of 8,497 eyes with open globe injury found that the most common injury type was penetrating injury with intraocular foreign body (IOFB) 1). In children, the incidence is reported as 11.8 per 100,000 per year, with over 35% of injuries occurring in children.
Penetrating injury refers to a wound with an entry site but no exit site. Perforating injury has both an entry and an exit wound, completely traversing the eye. Penetrating injuries are relatively less severe, but attention must be paid to the possibility of intraocular foreign body (IOFB).
In penetrating ocular trauma, there is only an entry wound, so there is no extrusion of intraocular contents into the posterior segment, and anterior segment findings are the main focus.
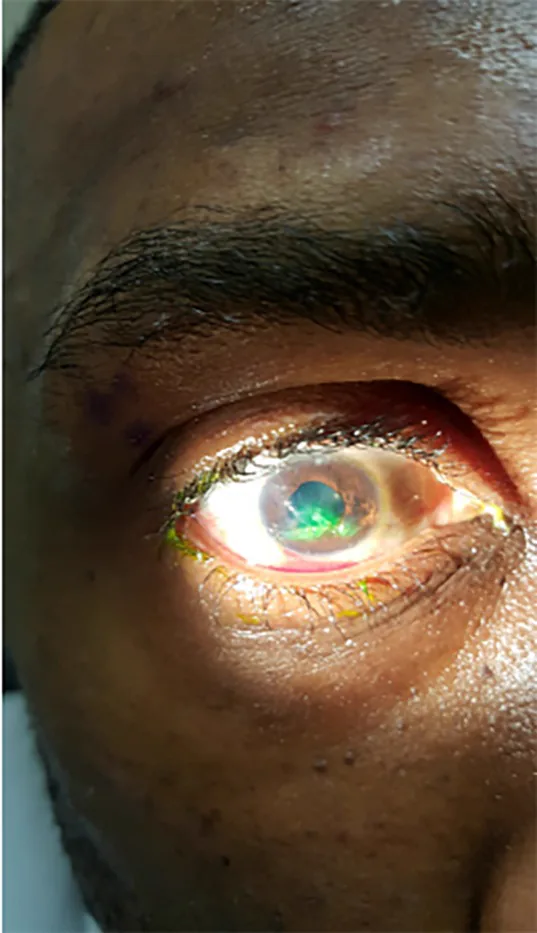
The Seidel test using fluorescein staining is useful for evaluating full-thickness wounds. Under cobalt blue light, aqueous humor leakage washes away the dye (Seidel positive), confirming a full-thickness wound.
The home and workplace are the most common locations of injury. The main causes are listed below.
Intraocular foreign bodies (IOFB) can complicate penetrating trauma. Metal fragments are most common, but wood and glass fragments are also causes.
The frequency of endophthalmitis in open globe injuries is 2–7%. Infections, especially from plants or soil, often lead to blindness. Unlike postoperative endophthalmitis after cataract surgery, endophthalmitis can be caused by virulent organisms such as Bacillus species. In orbital foreign bodies, anaerobic infections (e.g., tetanus) should also be considered.
Diagnosis of open globe injury involves a combination of detailed history taking, careful examination, and imaging studies. In penetrating ocular trauma, suspect retained foreign bodies, and consider CT if examination is insufficient or if intraocular foreign body (IOFB) is suspected 4).
Obtain detailed information on the time, mechanism, and causative object of the injury. Also check for use of protective or prescription glasses, tetanus immunization status, and time of last meal (due to possible general anesthesia). In patients with reduced consciousness, gathering information from family or associates is important. If emergency surgery under general anesthesia is anticipated, secure peripheral intravenous access and instruct the patient to fast.
| Imaging modality | Main indications | Notes |
|---|---|---|
| Orbital CT | Detection of IOFB, globe deformity, orbital fracture | Non-contrast orbital or facial CT is standard 4) |
| B-mode ultrasound | Posterior segment evaluation when view is poor | Avoid pressure if open globe is suspected |
| X-ray | Simple detection of metallic foreign bodies | Detectable if length ≥2 mm and thickness ≥0.4 mm |
| MRI | Non-metallic foreign bodies (e.g., wood) | Contraindicated if magnetic metal is suspected |
In penetrating ocular trauma with an entry wound, suspect a foreign body. CT can simultaneously evaluate intraocular foreign bodies (IOFB), globe deformation, orbital fractures, and intracranial lesions, making it useful when assessment by clinical findings alone is difficult 4).
If there is an entry wound, suspect retained foreign body. Even if anterior segment findings appear normal, an intraocular foreign body may be present. CT evaluation of the presence and location of foreign bodies, globe deformation, and orbital fractures is important; missing these can lead to delayed surgery or blindness 4).
The priority in treating penetrating ocular trauma is wound closure (primary repair) to prevent infection and extrusion of ocular contents.
Aim for primary repair within 24 hours of injury. A systematic review (8497 eyes, 15 studies) showed that repair within 24 hours significantly reduced the risk of endophthalmitis compared to delayed repair (OR 0.39, 95% CI 0.19-0.79, P=0.01)1). However, no significant difference in final visual acuity was observed based on repair timing (OR 0.89, 95% CI 0.61-1.29, P=0.52)1). General anesthesia is typically used.
Use 10-0 nylon. Aim for watertight closure, but avoid overtightening sutures to prevent corneal astigmatism or irregular astigmatism; take longer bites. Tighten all sutures evenly to prevent aqueous leakage.
Use 7-0 nylon (6-0 to 8-0 nylon also acceptable). First, secure the four rectus muscles to locate the wound. If the wound is deep and the rectus muscle obstructs, temporarily detach the tendon. Once a part of the rupture is found, suture sequentially from the easiest area to ensure closure. For limbal wounds, first suture with 9-0 nylon, then close the corneal wound with 10-0 nylon and the scleral wound with 9-0 nylon using interrupted sutures.
Management of iris incarceration depends on the extent of damage and contamination.
Start systemic broad-spectrum antibiotics covering gram-positive and gram-negative bacteria preoperatively. Combination of vancomycin and a third-generation cephalosporin (e.g., ceftazidime) is associated with reduced endophthalmitis rates. If endophthalmitis is suspected, early invasive treatment is recommended. Inject vancomycin 1 mg/0.1 mL and ceftazidime 2.25 mg/0.1 mL into the anterior chamber and vitreous. If vitreous opacification is extensive, perform emergency vitrectomy.
Once the presence of an intraocular foreign body is confirmed, it should be removed as soon as possible. Removal is primarily performed via pars plana vitrectomy using microforceps or diamond forceps. Detailed treatment strategies for intraocular foreign bodies are covered in the article on intraocular foreign bodies (IOFB).
Depending on the extent of damage to intraocular tissues, lensectomy and vitrectomy may be performed as secondary surgery. In cases of penetrating injury limited to the anterior segment, this may often be unnecessary. However, in the following situations, consider performing it as a single-stage procedure immediately following primary repair:
Primary repair should be aimed for within 24 hours of injury. A systematic review has shown that repair within 24 hours significantly reduces the risk of endophthalmitis (OR 0.39, 95% CI 0.19-0.79)1). However, no significant difference in final visual acuity has been found based on the timing of repair within 24 hours.
If the prolapse is within 6 to 8 hours and there is no severe contamination, attempt iris repositioning. If the tissue is necrotic or heavily contaminated, choose iridectomy. Both procedures must be performed in the operating room; bedside manipulation is contraindicated.
Penetrating ocular trauma occurs when a sharp object penetrates the eye wall at high speed. It tends to occur at the thinnest parts of the sclera, such as the limbus and posterior to the rectus muscle insertions. Unlike perforating injuries, there is no exit wound, so the eye shape is somewhat preserved without posterior extrusion of intraocular contents. Anterior extrusion (iris incarceration) is the main feature.
Iris incarceration at the laceration site results in a pear-shaped pupil. The incarcerated iris seals the anterior chamber anteriorly, but if left untreated for a long time, the risk of iris tissue necrosis and infection increases.
There are two mechanisms of retinal detachment in penetrating ocular trauma.
The following secondary changes may occur after initial treatment of the trauma.
McMaster et al. (2025) conducted a systematic review and meta-analysis on the timing of primary repair after open globe injury and its association with visual outcomes and endophthalmitis rates 1). The study included 8497 eyes (15 studies), with the most common injury type being penetrating injury combined with IOFB. Repair within 24 hours reduced the risk of endophthalmitis compared to delayed repair (OR 0.39, 95% CI 0.19-0.79, P=0.01). However, no significant difference in final visual acuity was observed based on repair timing (OR 0.89, 95% CI 0.61-1.29, P=0.52). All included studies were retrospective and non-randomized, with the certainty of evidence rated as low to very low.
The Ocular Trauma Score (OTS) is a prognostic tool that estimates the probability of visual outcomes based on initial visual acuity, presence of globe rupture, endophthalmitis, penetrating injury, retinal detachment, and relative afferent pupillary defect (RAPD). In penetrating ocular trauma, prognosis can be stratified by combining visual acuity, RAPD, and injury zone.
Kheir et al. (2021) reported 48 eyes of 39 patients with ocular trauma following the Beirut port explosion 2). Open globe injury was found in 20.8%, hyphema in 18.8%, and surface injuries (conjunctival laceration, corneal laceration) in 54.2%. Due to the nature of explosive devices causing multiple tiny fragments to penetrate simultaneously, penetrating injuries are common and often complicated by multiple IOFBs. In civilian and military blast incidents, CT is crucial for detecting IOFBs.
McMaster D, Bapty J, Bush L, Serra G, Kempapidis T, McClellan SF, et al. Early versus Delayed Timing of Primary Repair after Open-Globe Injury: A Systematic Review and Meta-analysis. Ophthalmology. 2025;132(4):431-441. doi:10.1016/j.ophtha.2024.08.030. PMID:39218161.
Kheir WJ, Awwad ST, Bou Ghannam A, Khalil AA, Ibrahim P, Rachid E, El Salloukh NA, Yehia M, et al. Ophthalmic Injuries After the Port of Beirut Blast-One of Largest Nonnuclear Explosions in History. JAMA ophthalmology. 2021;139(9):937-943. doi:10.1001/jamaophthalmol.2021.2742. PMID:34351374; PMCID:PMC8343520.
Germerott T, Mann N, Axmann S. Penetrating eye injury by dart. Int J Legal Med. 2021;135(2):573-576. PMID: 33336294.
Zhou Y, DiSclafani M, Jeang L, Shah AA. Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls. Clinical Ophthalmology. 2022;16:2545-2559. doi:10.2147/OPTH.S372011. PMID:35983163; PMCID:PMC9379121.