A ruptured globe is an open-globe injury in which the eye wall is torn due to a sudden increase in intraocular pressure from blunt external force, leading to prolapse or incarceration of intraocular contents. Typical mechanisms include blunt trauma from a fist or ball, and it is one of the ophthalmic emergencies that significantly impairs visual function.
Open-globe injuries are broadly classified into penetrating injuries caused by sharp external force and ruptured globes caused by blunt external force. The mechanisms of injury and wound formation differ, and treatment strategies also differ.
The BETT (Birmingham Eye Trauma Terminology) is widely used for classifying ruptured globes.
Classification
Mechanism of Injury
Formation of Open Wound
Penetrating injury
Sharp external force (e.g., knife, nail)
Open wound directly at the site of external force
Ruptured globe
Blunt external force (e.g., fist, ball)
Indirect rupture at the thinnest part of the eye wall due to increased intraocular pressure
In a ruptured globe, increased intraocular pressure and shock waves create a scleral open wound parallel to the limbus. It is characterized by the absence of surface wounds on the cornea or conjunctiva, and it may be overlooked.
Zone Classification (International Ocular Trauma Classification)
The estimated incidence of ocular trauma is 3.5 to 4.5 per 100,000 population1). Severe ocular trauma in children occurs at a rate of 11.8 per 100,000 children per year, and children (mostly under 12 years old) account for more than 35% of severe ocular trauma. Common causes include sports, toys, falls, and violence.
QWhat is the difference between globe rupture and penetrating injury?
A
Globe rupture is an indirect break of the eyewall due to increased intraocular pressure from blunt trauma such as a fist or ball. Penetrating injury is a direct perforation of the eyewall by a sharp object such as a knife or nail. In the former, the open wound may be hidden under the conjunctiva and easily missed, making diagnosis difficult.
Relan M, et al. Globe Rupture – A Case Report and Review of Emergency Department Diagnosis and Management. Cureus. 2022. Figure 1. PMCID: PMC9637430. License: CC BY.
In the right eye of an elderly patient, dark red uveal tissue protruding from the corneal limbus and extensive periorbital hemorrhage are seen. This corresponds to ocular content prolapse and uveal prolapse discussed in the section “2. Main symptoms and clinical findings”.
Clinical findings of globe rupture are diverse. Acute vision loss and eye pain after trauma are common chief complaints, but findings vary greatly depending on the severity and location of the injury.
Typical findings of globe rupture
Severe conjunctival hemorrhage and edema: One of the most important findings suggesting globe rupture.
Subjective symptoms typically include sudden vision loss and severe eye pain immediately after trauma. In severe cases with extrusion of intraocular contents, vision often becomes light perception or worse.
Clinical features: It is often difficult to fully assess the injury through outpatient examination alone. Especially in blunt trauma, even if no external wound is apparent, the presence of extreme hypotony, severe conjunctival hemorrhage, edema, hyphema, or vitreous hemorrhage should strongly raise suspicion for open globe injury.
Specific signs of globe rupture include pupillary distortion and deformation (D-shaped pupil due to iris prolapse).
QCan globe rupture be missed?
A
Yes. In blunt trauma, the open wound may be hidden under the conjunctiva, making its location and size unclear. It may be covered by severe conjunctival hemorrhage and edema, and only present with hyphema and hypotony, leading to missed diagnosis. If significant hypotony is present after trauma, open globe injury should always be suspected and imaging performed.
Globe rupture is caused by blunt trauma. Understanding the mechanism of injury and risk factors is important for developing preventive measures.
Causes of blunt trauma:
Sports-related: Boxing (fist), baseball/softball (ball), tennis/squash (ball/racket), martial arts
Traffic accidents: Impact to the face from airbag deployment, collision with dashboard/steering wheel
Falls: Especially in the elderly
Explosive trauma: In the Beirut port explosion (2020), 48 eyes of 39 patients were analyzed, and 10 eyes (20.8%) were diagnosed with open globe injury. Surgical intervention was required in 53.8% 2)
Children: Accidents with toys (especially those with sharp points), playground equipment, collisions with peers
Risk factors:
Conditions that cause thinning and weakening of the sclera make the eyeball prone to rupture even with relatively minor trauma.
High myopia: Scleral thinning due to axial elongation
Aging: Scleral weakening
History of eye surgery: Cataract surgery wounds, corneal transplant wounds, and glaucoma surgery wounds are relatively fragile and may rupture with minor blunt trauma
Explosive trauma involves a combination of primary injury (pressure wave from blast), secondary injury (fragments and debris), and tertiary injury (body displacement by blast wind), often accompanied by open globe injury, optic nerve damage, and orbital fractures 2).
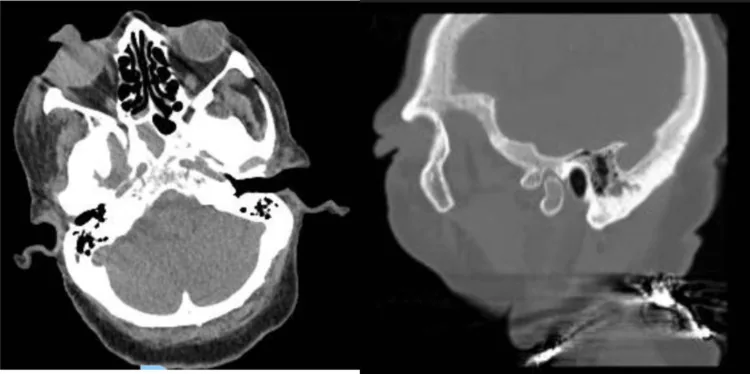
Relan M, et al. Globe Rupture – A Case Report and Review of Emergency Department Diagnosis and Management. Cureus. 2022. Figure 2. PMCID: PMC9637430. License: CC BY.
Axial view (left) shows deformity of the right globe and high-density areas in the orbital soft tissues; sagittal view (right) shows uveal tissue prolapse anteriorly. This corresponds to the CT evaluation of globe rupture discussed in section “4. Diagnosis and Examination Methods.”
A systematic approach is necessary for diagnosing globe rupture. It is uncommon to fully grasp the extent of injury through outpatient examination alone; imaging studies should be actively utilized.
Intraocular pressure measurement is contraindicated: If open globe injury is suspected, any maneuver that compresses the globe should be avoided. Only simple assessment by finger palpation is allowed.
Avoid using a lid speculum: It may promote extrusion of intraocular contents.
Slit-lamp examination: Perform if possible. Check for hyphema, iris prolapse, and lens dislocation.
Minimize contact with the eye when perforation is suspected
CT is excellent for confirming metallic foreign bodies and assessing ocular morphology, and is the first-choice imaging test in cases of suspected globe rupture. MRI is useful for precise evaluation of non-metallic foreign bodies (e.g., wood, plastic), but MRI is absolutely contraindicated if a metallic foreign body is suspected 1).
Prognosis prediction using the Ocular Trauma Score (OTS)
OTS is useful as a prognostic score for open globe injuries at initial presentation. Initial visual acuity, zone classification, RAPD, presence of retinal detachment, and type (penetrating vs. rupture) are scored to predict final visual acuity1). A lower OTS score indicates a worse visual prognosis and can be used to guide treatment decisions and patient counseling.
Hyphema only, integrity of the eyewall is preserved
QWhat is the most important test for diagnosing a ruptured globe?
A
CT is the priority examination. It allows assessment of eyewall integrity, intraocular foreign bodies, and orbital fractures, and is excellent for detecting metallic foreign bodies. MRI is useful for precise evaluation of non-metallic foreign bodies but is absolutely contraindicated when a metallic foreign body is suspected. Intraocular pressure measurement and use of a lid speculum are avoided as they compress the globe.
The purpose of primary surgery is to prevent infection and extrusion of ocular contents.
Primary surgery (wound closure)
Anesthesia selection: For small wounds limited to the cornea and anterior segment, local anesthesia with retrobulbar block may be used. If wound identification is difficult due to bleeding or edema, general anesthesia is selected.
Suture materials: 10-0 nylon suture for corneal wounds, 7-0 nylon suture for scleral wounds.
Repositioning of prolapsed tissue: Reposition uveal tissue and vitreous, then close the wound with sutures.
Wound exploration: If the wound is unclear, incise the conjunctiva and systematically explore near the extraocular muscle insertions, the thinnest part of the sclera.
A systematic review and meta-analysis of 8,497 eyes showed that primary repair within 24 hours significantly reduces the risk of endophthalmitis compared to delayed repair beyond 24 hours (endophthalmitis rate: 11% in the ≤24-hour group vs. 28% in the >24-hour group; OR 0.39, 95% CI 0.19–0.79, P=0.01)1).
On the other hand, no significant difference in visual prognosis was found between primary repair within 24 hours and delayed repair (OR 0.89, 95% CI 0.61–1.29, P=0.52)1). However, severe cases tend to be seen and operated on earlier, so attention to selection bias is necessary1). Currently, primary repair within 24 hours is recommended.
In addition to preoperative systemic antibiotic administration, intravitreal antibiotic injection during the second surgery may also be performed for infection prevention. The specific choice and dosage of antibiotics are determined based on the severity of the case, contamination status, and risk of resistant bacteria.
QBy when should surgery be performed?
A
A meta-analysis (8,497 eyes) showed that primary repair within 24 hours significantly reduces the risk of endophthalmitis compared to repair after 24 hours (11% vs 28%, OR 0.39) 1). Repair within 24 hours is recommended. However, decisions should be made based on the facility and patient condition, and systemic status may take priority in some cases.
QWhat is the prognosis for globe rupture?
A
Prognosis depends largely on the extent of associated injuries. Some cases rapidly progress to phthisis bulbi postoperatively, so the outlook is not optimistic. In addition to the risks of endophthalmitis and tractional retinal detachment, attention must be paid to sympathetic ophthalmia (which can also endanger the healthy fellow eye), and long-term follow-up is essential.
When blunt trauma is applied to the eye, intraocular pressure rises sharply. Since the eye is a closed space, pressure is transmitted in all directions, and rupture occurs at the thinnest part of the ocular wall. The thinnest areas are the limbus (corneoscleral junction) and the sclera near the extraocular muscle insertions, where open wounds are likely to form.
A key difference between blunt trauma and penetrating trauma is that in penetrating trauma, a sharp object creates an open wound directly at the site of external pressure, whereas in globe rupture, the rupture occurs indirectly at the thinnest part of the ocular wall. Therefore, the open wound in globe rupture is often located away from the impact site, especially in subconjunctival areas that are difficult to see.
Shock waves from blunt trauma propagate throughout the eye and may cause retinal and choroidal damage on the side opposite the impact site. Thus, retinal damage, choroidal rupture, and optic nerve injury may occur at sites distant from the direct open wound.
Ocular contents (uveal tissue, vitreous, lens) may extrude and become incarcerated in the open wound. The principle of primary surgery is to reposition incarcerated tissue without careless excision.
Globe rupture due to explosion presents with complex injury mechanisms. Analysis of the Beirut port explosion showed a combination of primary injury (blast pressure wave), secondary injury (fragmentation), and tertiary injury (body displacement). Among 48 eyes of 39 patients, 10 eyes (20.8%) had open globe injuries, and 53.8% required surgical intervention 2). The presence of foreign bodies and multiple traumas are characteristic of explosive injuries, requiring systematic evaluation and multidisciplinary collaboration.
Although repair within 24 hours is recommended, current evidence is based on retrospective studies, and the GRADE assessment is low 1). Conducting prospective randomized controlled trials (RCTs) is a future challenge. Studies that eliminate the influence of selection bias (more severe cases tend to seek early medical attention and surgery) are needed.
Prospective data collection through the IGATES registry
The IGATES (International Globe and Adnexal Trauma Epidemiology Study) registry is a project aimed at international prospective data collection on open globe injuries. The accumulated data is expected to enable the construction of more accurate prognostic models and the establishment of optimal treatment strategies 1).
Improvement of OTS and enhancement of prognostic accuracy
Further refinement of the Ocular Trauma Score (OTS) and validation of its external validity are underway. Improving prognostic accuracy at the initial examination is important for both treatment decision-making and patient counseling.
Optimal regimen for prophylactic antibiotic administration
There is a lack of unified evidence regarding the optimal type, dose, and duration of antibiotic administration before, during, and after surgery, and this remains a topic for future research.
Development of ophthalmic response protocols for disasters
The report on the Beirut port explosion highlighted the importance of ophthalmic trauma response in large-scale explosion disasters. Establishing disaster medical systems involving ophthalmologists and developing protocols for managing explosive eye injuries are recognized as international challenges 2).
Research on prevention of proliferative vitreoretinopathy (PVR)
Proliferative vitreoretinopathy (PVR) is a major complication after globe rupture. Research on drugs and surgical techniques aimed at preventing PVR is ongoing, with efforts to improve functional outcomes.
McMaster D, Bapty J, Bush L, Serra G, Kempapidis T, McClellan SF, Woreta FA, Justin GA, et al. Early versus Delayed Timing of Primary Repair after Open-Globe Injury: A Systematic Review and Meta-analysis. Ophthalmology. 2025;132(4):431-441. doi:10.1016/j.ophtha.2024.08.030. PMID:39218161.
Kheir WJ, Awwad ST, Bou Ghannam A, Khalil AA, Ibrahim P, Rachid E, El Salloukh NA, Yehia M, Torbey J, El Zein L, Jabbur NS, Noureddin B, Alameddine RM.. Ophthalmic Injuries After the Port of Beirut Blast-One of Largest Nonnuclear Explosions in History. JAMA Ophthalmol. 2021;139(9):937-943. doi:10.1001/jamaophthalmol.2021.2742. PMID:34351374; PMCID:PMC8343520.
Mahmoud TH, Govindaraju VK. Primary Repair of Ruptured Globe on No Light Perception Eyes and the Role of Vitreoretinal Surgery. Ophthalmol Retina. 2024;8(7):615-616. PMID: 38969437.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.