The Seidel test is a diagnostic method that detects aqueous humor leakage from a full-thickness defect in the cornea or sclera by applying fluorescein dye to the ocular surface and observing under cobalt blue light. It was reported in 1921 by the German ophthalmologist Erich Seidel (1882–1948).
When aqueous humor leaks from a defect, it dilutes the fluorescein dye applied to the ocular surface. Under cobalt blue light, a dark blue stream (waterfall effect) appears within the green fluorescence of fluorescein. This is a positive Seidel test.
QWhat kind of test is the Seidel test?
A
It is a test that detects aqueous humor leakage by observing the ocular surface after applying fluorescein dye under cobalt blue light. If there is a full-thickness defect in the cornea or sclera, aqueous humor dilutes the fluorescein and appears as a dark blue stream. It is used for trauma, infection, and postoperative wound closure evaluation.
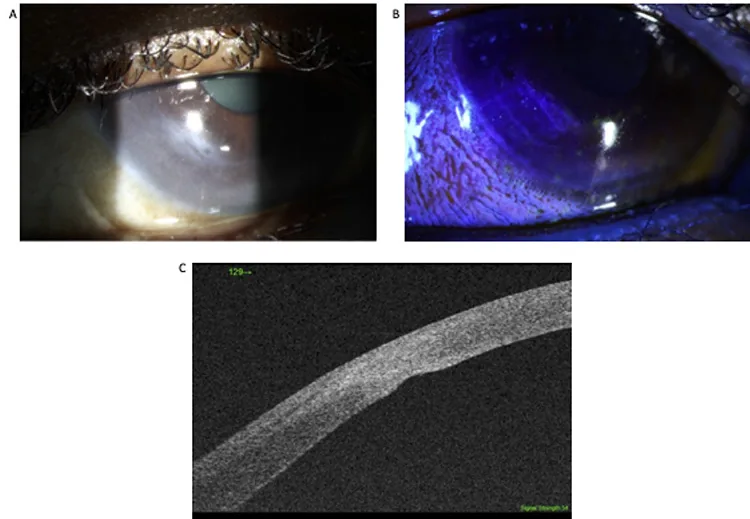
Papamlichael E, Logeswaran A, Papastefanou VP, et al. Evaluation and management of a spontaneous corneal rupture secondary to pellucid marginal degeneration, using swept-source anterior segment optical coherence tomography. Oxford Medical Case Reports. 2021 Mar 8; 2021(3):omab003. Figure 4. PMCID: PMC7947267. License: CC BY.
Slit-lamp and fluorescein staining show aqueous humor leakage from the wound, and anterior segment OCT shows a cross-section of wound dehiscence. The finding of aqueous humor outflow through the wound is correlated between clinical image and tomographic image.
In the diagnosis of traumatic hyphema, the Seidel test is performed to confirm the presence or absence of corneal perforation. If severe conjunctival edema, low intraocular pressure, or subconjunctival hemorrhage is observed, suspect globe rupture and add imaging tests (CT, MRI). However, MRI is contraindicated if a metallic foreign body is suspected.
This is also an important test in the evaluation of blebs after trabeculectomy. Apply fluorescein test paper soaked with topical anesthetic to the bleb surface and observe the entire area under a blue-free filter. It is easier to detect leakage by having the patient close the eye and then observing for a few seconds immediately after opening. In blebs after concomitant use of antimetabolites, the wall becomes thin and the risk of aqueous humor leakage is high.
Fluorescein is a water-soluble fluorescent dye. Its maximum absorption wavelength is around 490 nm (blue light), and its maximum fluorescence wavelength is 520–530 nm (green light). When excited by a cobalt blue filter, it emits yellow-green fluorescence.
In the normal corneal epithelium, tight junctions of superficial cells act as a barrier, so fluorescein does not pass between cells. In areas of epithelial defect, fluorescein enters and stains the tissue. This property is also widely used to detect corneal and conjunctival epithelial disorders.
When there is a full-thickness defect in the cornea or sclera, aqueous humor leaks from the anterior chamber through the defect. The leaked aqueous humor dilutes fluorescein on the ocular surface and is observed as a dark blue stream (waterfall effect) under cobalt blue light. This is a positive finding.
Using a blue-free filter selectively transmits only the fluorescence wavelength of fluorescein (520–530 nm or longer), improving contrast and increasing the detection accuracy of subtle leaks.
1. Patient positioning: Have the patient sit in front of the slit lamp microscope.
2. Topical anesthesia: Administer topical anesthetic drops.
3. Drying: Carefully dry the suspected leak site with a cellulose sponge (recommended) or a cotton swab.
4. Fluorescein application: Moisten a fluorescein strip with saline and apply it to the suspected site. Alternatively, a drop of fluorescein solution (0.5–2%) may be used.
Observation and Evaluation
5. Observation: Observe the defect under cobalt blue light and evaluate for the presence of a dark stream (waterfall effect). Record the flow rate. Using a blue-free filter improves contrast.
6. Compression test: In certain cases, such as postoperative wounds, gently compress the area adjacent to the defect to confirm leakage. However, avoid this if there is a risk of intraocular content extrusion.
Obvious globe rupture: Compression or manipulation may cause extrusion of intraocular contents.
Fluorescein hypersensitivity: Rare but a contraindication.
QWhen is the compression test performed?
A
In cases of suspected slow leakage, such as from a postoperative wound or a bleb after trabeculectomy, apply gentle pressure to confirm the leak. However, in traumatic cases with risk of intraocular content extrusion, pressure must be avoided.
Traumatic full-thickness laceration/perforation: This constitutes an open globe injury and requires prompt surgical repair.
Large corneal defect: Perform primary suture closure. In post-LASIK corneas, a flap-related laceration may be present, requiring lifting of the flap and suturing of the residual stroma 2).
Conservative Management
Small perforation (less than 2 mm): May be managed with a bandage contact lens and antibiotic eye drops.
Cyanoacrylate adhesive: Used for small corneal defects.
Postoperative slow leakage: May be managed with a bandage contact lens and observation, expecting spontaneous closure.
QWhat to do if the Seidel test is positive?
A
Management varies depending on the cause, location, and size. Traumatic full-thickness lacerations or perforations require prompt surgical repair. Small perforations (less than 2 mm) or postoperative slow leakage may be managed with a bandage contact lens and antibiotics. Cyanoacrylate adhesive is also used for small defects.
6. False Positives, False Negatives, and Limitations
In eyes with a glaucoma drainage device (GDD), the lacrimal duct opening is close to the superior temporal conjunctiva around the device. Secretions from the lacrimal duct can dilute fluorescein and be mistaken for GDD leakage, resulting in a false positive (pseudo-Seidel sign) 1).
Fluorescein staining can detect fluid outflow, but it cannot distinguish whether the fluid is aqueous humor or tears. To overcome this limitation, a method has been reported in which trypan blue is injected into the anterior chamber to differentiate by whether the leaked fluid is colored blue 1). Trypan blue has high affinity for the conjunctiva, sclera, and trabecular meshwork, allowing accurate tracking of aqueous humor flow 1).
In eyes after LASIK, even if blunt trauma causes a full-thickness corneal stromal laceration, the LASIK flap may remain intact, preventing aqueous humor from leaking out, and the Seidel test may be negative 2). In such cases, a double chamber forms between the anterior chamber and the flap, presenting as corneal edema or low intraocular pressure2). There are reports where anterior segment OCT visualized the laceration under the flap and led to the diagnosis 2).
Even in cases of corneal ulcer perforation, fluorescein staining can visualize aqueous humor leakage, but if the perforation is self-sealed or temporarily stopped by iris incarceration, a false negative may occur.
QCan the Seidel test be false negative?
A
Yes. In eyes after LASIK, the intact flap may cover a full-thickness stromal laceration and prevent aqueous leakage, leading to a false negative 2). Iris incarceration or self-sealing of the perforation can also cause false negatives. If there is inconsistency with clinical findings, additional evaluation with anterior segment OCT is recommended.
Mahmud H, Mesfin Y, Liu Y, Ou Y, Lu JE. The use of trypan blue to distinguish Pseudo-Seidel sign from lacrimal ductule versus glaucoma drainage device leakage. American journal of ophthalmology case reports. 2025;39:102389. doi:10.1016/j.ajoc.2025.102389. PMID:40703767; PMCID:PMC12284709.
Pirhadi S, Adnani SY, Jadidi K. Unusual presentation of corneal laceration in a post-LASIK eye following blunt trauma. Am J Ophthalmol Case Rep. 2022;26:101419.