Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease that predominantly affects areas with apocrine sweat glands. It is characterized by painful nodules, abscesses, and fistulas, occurring in the axillae, groin, buttocks, and under the breasts. The estimated global prevalence ranges from 0.00033% to 4.1%, with reports of 0.7% to 1.2% in Europe and the United States.
Although HS is a skin disease, systemic inflammation can also affect the eyes. Approximately 13.89% of HS patients have some ocular findings. The most common ocular complication is uveitis, followed by scleritis and keratitis. Another study reported that episcleritis showed the strongest association.
The pathogenesis of HS primarily involves occlusion of the pilosebaceous unit 2). Subsequent follicular rupture and immune response trigger an inflammatory cascade, leading to systemic elevation of inflammatory cytokines such as TNF, IL-1, IL-17, and IL-23 2). These cytokines are also deeply involved in the pathogenesis of uveitis and dry eye1), and are considered to partly explain the mechanism of ocular complications in HS.
HS shares some immunological mechanisms with spondyloarthritis-related immune diseases such as psoriasis, Crohn’s disease, and ulcerative colitis, as well as vasculitides such as Behçet’s syndrome and systemic lupus erythematosus. Ocular complications are well known in these diseases, and a similar risk exists in HS.
QIf diagnosed with hidradenitis suppurativa, should I also see an ophthalmologist?
A
Because hidradenitis suppurativa (HS) involves systemic inflammation, ocular complications can occur. Even without symptoms, regular ophthalmologic screening is recommended. If symptoms such as redness, pain, blurred vision, or photophobia appear, please see an ophthalmologist promptly. Collaboration between dermatologists and ophthalmologists is important.
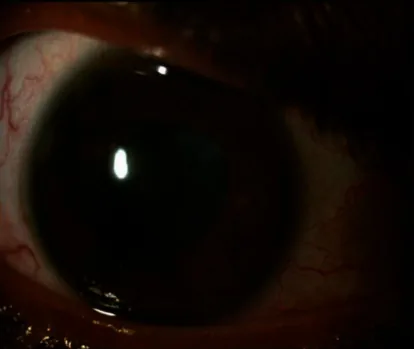
Ritasman Baisya, Meghna Gavali, Mudit Tyagi, Phani Kumar Devarasetti A Case of SAPHO Syndrome Complicated by Uveitis with Good Response to Both TNF Inhibitor and JAKinib 2023 Jan 18 Case Rep Rheumatol. 2023 Jan 18; 2023:6201887 Figure 3. PMCID: PMC9876693. License: CC BY.
Right eye showing irregular pupil due to posterior synechiae, poor dilation, and lens opacity. Anterior segment photograph showing anterior chamber inflammation with complicated cataract.
Retinal vascular changes: On OCTA, decreased foveal VD and VLD, as well as decreased VD in the deep retinal capillary plexus, have been reported.
Periorbital lesions: Rarely, HS lesions may appear on the face and eyelids.
Studies using OCTA have detected retinal microvascular abnormalities even in HS patients without clinical eye disease. These findings are similar to those seen in diabetic retinopathy and are thought to reflect the comorbid risk of HS and type 2 diabetes.
QHow often do ocular symptoms occur in hidradenitis suppurativa?
A
Approximately 13.89% of HS patients are reported to have ocular findings. Uveitis is the most common, followed by scleritis/episcleritis and keratitis. However, since studies on these ocular complications included patients with other autoimmune diseases, the exact frequency in HS alone has not yet been established.
The primary defect in the pathogenesis of HS is follicular occlusion of the pilosebaceous unit 2). Histologically, early findings include infundibular acanthosis, hyperkeratosis, and perifollicular immune cell infiltration 2). The immune response following follicular rupture triggers an inflammatory cascade, leading to the formation of nodules, abscesses, and fistulas.
In the study by Fitzsimmons and Gilbert, HS aggregation was observed in 14 out of 23 families, and 30% of patients had a strong family history. Abnormalities in the Notch signaling pathway are involved, and mutations in the PSENEN, KRT5, POFUT1, and POGLUT1 genes have been reported 3). Since the Notch pathway is also involved in melanocyte homeostasis and hair follicle differentiation control, its abnormalities may affect not only the skin but also multiple organs 3).
TNF, IL-1, IL-17, and IL-23 are elevated in the skin and serum levels 2). Among these cytokines, TNF-α and IL-6 are deeply involved in the pathogenesis of uveitis and correlate with ocular pain in dry eye1). Epithelial cells release TNF-α, IL-1, IL-6, and IL-8, amplifying the immune response and attracting inflammatory cells 1).
Lithium can directly act on hair follicle keratinocytes and induce HS through neutrophil migration and phagocytosis promotion 4). Discontinuation of lithium improves skin symptoms 4).
Ocular inflammation associated with Crohn’s disease
Differentiation from Crohn’s disease is particularly important. HS and Crohn’s disease coexist in 17–40% of patients 2) and share similar immune dysregulation. Treatment response may also provide diagnostic clues. If ocular symptoms improve after systemic therapy targeting HS-specific cytokines, it supports the diagnosis.
In HS patients with ophthalmic comorbidities, it has been reported that they respond poorly to topical dermatological treatments but respond well to anti-TNF-α therapy. TNF-α is also involved in the early pathogenesis of uveitis1), and anti-TNF-α therapy has the advantage of simultaneously treating both skin and eye symptoms of HS.
There is also evidence that biologic users have a lower risk of conjunctivitis compared to non-users.
Anti-inflammatory steroid eye drops after infection control
QAre biologics effective for ocular symptoms of hidradenitis suppurativa?
A
Yes, anti-TNF-α therapy (adalimumab, infliximab) has been reported to be effective not only for skin symptoms but also for ocular inflammation. Since TNF-α is involved in the pathology of uveitis and dry eye, this treatment has the advantage of simultaneously treating both the skin and eyes of HS. In HS patients with ophthalmic comorbidities, topical skin treatment alone is often insufficient, and systemic anti-TNF-α therapy is often required.
The pathology of HS begins with occlusion of the pilosebaceous unit 2). Early histological changes include infundibular acanthosis and hyperkeratosis, followed by lymphohistiocytic immune cell infiltration around the hair follicle. Rupture of the hair follicle causes leakage of keratin into the surrounding tissue, triggering a strong inflammatory response 2).
In this inflammatory process, TNF, IL-1, IL-17, and IL-23 are elevated in the skin and serum. These elevated cytokines expand perifollicular inflammation, progressing from abscess and nodule formation to draining fistulas.
Many of the cytokines elevated in HS are also involved in the pathology of ocular inflammation. TNF-α induces the expression of chemokines and adhesion molecules, prolonging inflammation in uveitis1). IL-6 is involved in intraocular immune responses in several types of uveitis and correlates with ocular pain in dry eye1).
A review by Rojas-Carabali et al. showed that epithelial cells produce and release TNF-α, IL-1, IL-6, and IL-8, amplifying the immune response and promoting the attraction of inflammatory cells in dry eye1).
Furthermore, IP-10/CXCL10 is a chemokine released from leukocytes, neutrophils, eosinophils, monocytes, and stromal cells in response to IFN-γ, and is also involved in intraocular inflammation 1).
Immunological Similarities Between HS and Crohn’s Disease
HS and Crohn’s disease share significant increases in IL-1, IL-6, IL-17, IL-23, and TNF 2). Both diseases are histologically characterized by lymphoid follicles and granulomas, and coexist in 17–40% of patients 2). Ocular complications are well known in inflammatory bowel disease including Crohn’s disease, and HS is thought to similarly affect the eyes through systemic inflammatory dysregulation.
Abnormalities in the Notch signaling pathway have attracted attention as a genetic background of HS. Mutations in PSENEN, a subunit of the γ-secretase complex, inhibit intracellular cleavage of Notch receptors 3). Disruption of the Notch pathway causes abnormal proliferation and differentiation of hair follicles, leading to epidermal hyperkeratosis and follicular occlusion. This mechanism explains the coexistence of Dowling-Degos disease and HS3).
Recent studies using OCTA have detected abnormalities in the retinal microvasculature even in HS patients without clinical eye disease. Decreases in foveal vessel density (VD) and vessel length density (VLD), as well as reduced VD in the deep retinal capillary plexus, have been reported, suggesting that HS may cause potential retinal vascular complications.
Anti-TNF-α therapy has shown efficacy for both skin and ocular symptoms of HS and is expected to continue playing a central role in treatment. As new biologic agents and JAK inhibitors are developed, verification of their effectiveness against HS ocular complications is anticipated.
The exact prevalence and pathogenesis of ocular complications in HS patients are not yet fully understood. Large-scale prospective studies are needed to identify the frequency and risk factors of HS-specific ocular symptoms and to establish optimal screening protocols.
Rojas-Carabali W, Mejía-Salgado G, Cifuentes-González C, et al. Clinical relationship between dry eye disease and uveitis: a scoping review. J Ophthalmic Inflamm Infect. 2023;13(1):2. doi:10.1186/s12348-022-00323-0. PMID:36715869; PMCID:PMC9886213.
Srisajjakul S, Prapaisilp P, Bangchokdee S. Magnetic Resonance Imaging of Hidradenitis Suppurativa: A Focus on the Anoperineal Location. Korean journal of radiology. 2022;23(8):785-793. doi:10.3348/kjr.2022.0215. PMID:35914743; PMCID:PMC9340234.
Dupont M, Parent M, Vanhooteghem O. About a Rare Association Between Vulvar Dowling Degos Disease and HS. International journal of women’s health. 2023;15:355-359. doi:10.2147/IJWH.S398604. PMID:36923583; PMCID:PMC10010119.
Chaudhari D, Vohra RR, Abdefatah Ali M, Nadeem H, Tarimci B, Garg T, et al. A Rare Phenomenon of Lithium-Associated Acne Inversa: A Case Series and Literature Review. Cureus. 2023;15(3):e36051. doi:10.7759/cureus.36051. PMID:37056525; PMCID:PMC10089641.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.