Superficial neovascularization

Corneal Neovascularization
1. What is corneal neovascularization?
Section titled “1. What is corneal neovascularization?”Corneal neovascularization (CoNV) is a condition in which new capillaries from the limbal vascular plexus invade the normally avascular corneal tissue 1). It is not a specific disease but a non-specific response to various conditions such as infection, inflammation, hypoxia, and trauma.
The cornea maintains a “corneal angiogenic privilege (CAP),” where the avascular state is preserved by a precise balance between angiogenic inhibitors and promoters 1). When this balance is disrupted, vascular endothelial cells proliferate, migrate, and invade the corneal stroma.
New blood vessels are classified into two types based on their anatomical location.
Deep stromal neovascularization
It invades from the anterior ciliary arteries into the corneal stroma.
It occurs due to persistent inflammation or edema in conditions such as interstitial keratitis (syphilis, tuberculosis), stromal herpes keratitis, and bullous keratopathy.
Immature new blood vessels cause lipid exudation, persistent inflammation, and scarring 1). As they progress, the vessels mature, become covered by pericytes, and become resistant to anti-VEGF therapy 1). In patients after corneal transplantation, new blood vessels are a risk factor for rejection.
Q
What happens if corneal neovascularization is left untreated?
A
If left untreated, the new blood vessels mature and become less likely to regress spontaneously, leading to lipid keratopathy (lipid deposition in the cornea) and corneal scarring, causing permanent vision loss. Additionally, if corneal transplantation becomes necessary, the presence of new blood vessels increases the risk of graft rejection. Early consultation and treatment of the underlying cause are important.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”Subjective Symptoms
Section titled “Subjective Symptoms”- Decreased vision: Occurs when neovascularization or its sequelae (lipid deposition, scarring) involve the visual axis
- Redness: Conjunctival injection associated with the underlying disease
- Asymptomatic: Often no subjective symptoms if the lesion does not involve the visual axis.
Clinical Findings (Findings Confirmed by Physician Examination)
Section titled “Clinical Findings (Findings Confirmed by Physician Examination)”- Morphology of new vessels: Varies from fine reticular patterns to engorged active vessels and mature high-density vessels.
- Location and depth of vessels: Assess whether superficial or deep using slit-lamp microscopy with slit and indirect illumination methods.
- Ghost vessel: An old blood vessel with no blood flow. No treatment is needed.
- Conjunctivalization: A condition where conjunctival tissue covers the cornea. It is confirmed by delayed staining with fluorescein.
- Lipid keratopathy: Yellow-white opacity caused by lipid leakage from new blood vessels depositing in the corneal stroma.
- Loss of Vogt’s palisades of Vogt (POV): An important finding suggesting loss of limbal stem cells.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Infectious Diseases
Section titled “Infectious Diseases”- Herpes simplex virus (HSV-1): The most common infectious cause of corneal neovascularization in developed countries 1). Stromal herpes keratitis leads to deep vascularization
- Bacterial keratitis: In severe cases, corneal ulceration and scarring are accompanied by vascular invasion
- Fungal keratitis: May be accompanied by corneal neovascularization in cases of delayed treatment
- Trachoma and onchocerciasis: Major infectious causes in developing countries1)
Hypoxia (contact lens-related)
Section titled “Hypoxia (contact lens-related)”Inappropriate over-wearing of soft contact lenses is the main cause. In approximately 80–90% of conventional HEMA material SCL wearers, vascular invasion from the superior cornea (10 to 2 o’clock direction) is observed. If epithelial damage persists for more than one month, blood vessels invade that area.
Chemical Trauma
Section titled “Chemical Trauma”Alkali injuries penetrate deep into the corneal stroma, causing extensive limbal stem cell damage and neovascularization. This is one of the groups with a significantly low success rate for corneal transplantation.
Limbal Stem Cell Deficiency (LSCD)
Section titled “Limbal Stem Cell Deficiency (LSCD)”LSCD is one of the major pathways for corneal neovascularization 1)3). When limbal stem cells become dysfunctional due to congenital causes, chemical trauma, contact lens overwear, systemic inflammatory diseases, or iatrogenic factors, the normal epithelial barrier is lost, leading to vascular invasion 3). In mild cases, fluorescein staining reveals whorl-like epitheliopathy; in moderate cases, superficial neovascularization and pannus appear 3).
Other Causes
Section titled “Other Causes”- Inflammatory diseases: SJS/TEN, ocular cicatricial pemphigoid, vernal keratoconjunctivitis, rosacea keratitis
- After corneal transplantation: Neovascularization due to rejection 1)
- Degenerative diseases: Terrien marginal degeneration, gelatinous drop-like corneal dystrophy
Q
Can proper use of contact lenses prevent corneal neovascularization?
A
Yes, it can often be prevented. One of the main causes of corneal neovascularization is oxygen deficiency due to contact lenses. By adhering to wearing time, using lenses with high oxygen permeability, and undergoing regular eye examinations, the risk can be significantly reduced.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”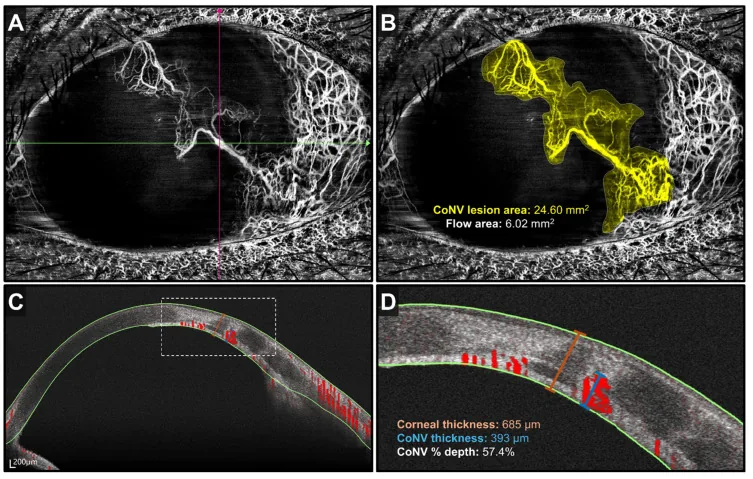
Brian Juin Hsien Lee, Kai Yuan Tey, Ezekiel Ze Ken Cheong, Qiu Ying Wong, et al. Anterior Segment Optical Coherence Tomography Angiography: A Review of Applications for the Cornea and Ocular Surface 2024 Sep 28 Medicina (Kaunas). 2024 Sep 28; 60(10):1597 Figure 1. PMCID: PMC11509466. License: CC BY.
A and B are OCTA en face images showing new blood vessels extending from the corneal periphery toward the center and the lesion area. C and D are cross-sectional images measuring the depth and thickness of new blood vessels running within the corneal stroma.
Slit-lamp microscopy
Section titled “Slit-lamp microscopy”This is the most basic test for diagnosing corneal neovascularization. It evaluates the location (quadrant), depth (superficial/deep), activity (presence of blood flow), and presence of conjunctival invasion of the blood vessels.
- Diffuser method: Widening the illumination beam or observing through a diffuser makes it easier to identify new blood vessels
- Indirect illumination: Observing new blood vessels and corneal nerves using reflected light from the iris or lens
- Fluorescein staining: Useful for assessing epithelial defects and conjunctival invasion
Fluorescein angiography
Section titled “Fluorescein angiography”- Fluorescein angiography (FA): Functionally evaluates vascular perfusion and leakage, distinguishing active from mature vessels1)
- Indocyanine green angiography (ICGA): Excellent for visualizing deep vessels and feeder vessels, useful for targeting vascular occlusion therapy1)
Imaging tests
Section titled “Imaging tests”- Anterior segment OCT / OCT-A: Noninvasively quantifies the depth and extent of corneal vascular networks1)
- In vivo confocal microscopy (IVCM): Enables quantification of epithelial basal cells in the diagnosis of LSCD3)
| Examination method | Main evaluation items | Features |
|---|---|---|
| Slit-lamp microscope | Location, depth, activity | First-choice basic test |
| FA / ICGA | Perfusion, leakage, feeder vessels | Useful for treatment planning |
| AS-OCT / OCT-A | Depth and quantitative assessment | Non-invasive |
5. Standard treatment
Section titled “5. Standard treatment”Treatment of corneal neovascularization consists of two main pillars: treatment of the cause and intervention for the neovascularization itself2).
Treatment of the cause
Section titled “Treatment of the cause”- Discontinuation of contact lens wear: In cases of hypoxia, discontinue lens wear and consider switching to a lens with higher oxygen permeability. Determine whether the vessels are active or old (ghost vessels).
- Treatment of infection: Administration of antibacterial, antiviral, or antifungal agents for the causative infectious keratitis.
- LSCD treatment: surgical treatments such as limbal transplantation and amniotic membrane transplantation
Pharmacotherapy
Section titled “Pharmacotherapy”- Steroid eye drops: suppress inflammatory cytokines (IL-1, IL-6), induce lymphocyte apoptosis, and inhibit vasodilation, thereby suppressing angiogenesis 2). First-line treatment, but caution is needed for steroid-induced glaucoma and increased susceptibility to infection with long-term use
- Anti-VEGF therapy: Bevacizumab (eye drops, subconjunctival injection, intrastromal injection) is widely used 1)2). Effective against immature active vessels, but limited effect on mature vessels (those covered by pericytes) 1). Since pericyte coverage reaches 80% within 2 weeks of neovascularization onset, early treatment is important 1)
- Immunosuppressive drugs: Cyclosporine A eye drops suppress T cell activation and have a steroid-sparing effect 2). Tacrolimus and sirolimus (mTOR inhibitor) are also options 1).
- Doxycycline: Inhibits corneal neovascularization through its anti-mucous membrane pemphigoid effect 2).
Surgical and Procedural Treatments
Section titled “Surgical and Procedural Treatments”- Laser photocoagulation: Coagulates and occludes blood vessels using argon or Nd:YAG laser. Used as a pretreatment before corneal transplantation and for treatment of lipid keratopathy. Risks include corneal hemorrhage and thinning; recanalization of vessels and formation of shunt vessels are often observed.
- Fine needle diathermy (FND): A thin needle is inserted into the feeder vessels of the limbus to electrically coagulate and occlude them. It is effective even for mature, thick vessels and is performed for afferent vessels that are difficult to occlude with argon laser1)
- Photodynamic therapy (PDT): After injecting a photosensitizer into the blood vessels, light irradiation generates reactive oxygen species that destroy the vessel walls. It has high specificity but is costly and time-consuming
- MICE (MMC intravascular chemoembolization): A technique in which mitomycin C (0.4 mg/mL) is directly injected into the feeder vessels using a 33-gauge needle6). For refractory corneal neovascularization resistant to conventional treatments, vascular ghosting and improvement of lipid keratopathy have been reported6)
6. Pathophysiology and Detailed Pathogenesis
Section titled “6. Pathophysiology and Detailed Pathogenesis”Maintenance Mechanisms of Corneal Angiogenic Privilege (CAP)
Section titled “Maintenance Mechanisms of Corneal Angiogenic Privilege (CAP)”The avascular state of the cornea is maintained by the coordinated action of multiple anti-angiogenic mechanisms1).
- Soluble VEGF receptor 1 (sVEGFR1): Constitutively produced by the corneal epithelium and stroma. It is an endogenous VEGF trap that captures VEGF-A with high affinity and competitively inhibits its binding to membrane-bound VEGFR1)
- Thrombospondin (TSP-1/TSP-2): Anti-angiogenic glycoproteins constitutively expressed in the corneal ECM. They sequester VEGF and suppress VEGFR2 signaling. They induce apoptosis of vascular endothelial cells (VECs) via CD36/CD471)
- Endostatin: A C-terminal fragment of collagen XVIII. It inhibits VEGF and bFGF pathways and promotes VEC apoptosis through increased caspase-3 activity. It also suppresses lymphangiogenesis1)
- Physical barriers: The limbal barrier, dense collagen arrangement, and relatively low temperature of the cornea restrict vascular invasion1)
Pro-angiogenic factors and pathogenic pathways
Section titled “Pro-angiogenic factors and pathogenic pathways”CAP breakdown occurs mainly through two pathways1)2).
Pathway 1: Increased production of promoting factors due to inflammation and hypoxia
Corneal injury causes the release of three major angiogenic factors from macrophages, epithelial cells, and endothelial cells1).
- VEGF-A: Promotes VEC proliferation and migration via VEGFR-2, induces MMP-2/MMP-9 to promote ECM remodeling1). It is the most important promoting factor in corneal neovascularization.
- bFGF (FGF-2): Enhances VEGF production via the ERK/PI3K pathway and dissociates VE-cadherin binding to promote VEC sprouting1)
- PDGF: Recruits pericytes and smooth muscle cells to stabilize new blood vessels1). PDGF-induced vascular maturation confers resistance to anti-VEGF therapy
Pathway 2: Limbal Stem Cell Deficiency (LSCD)
Loss of limbal stem cells disrupts the normal barrier function of the corneal epithelium, allowing conjunctival tissue invasion and persistent inflammation that sustain neovascularization1)3).
Relationship with lymphangiogenesis
Section titled “Relationship with lymphangiogenesis”Corneal neovascularization (angiogenesis) and lymphangiogenesis are interrelated but independent processes 4). Blood vessels function as the efferent pathway for immune effector cells, while lymphatic vessels serve as the afferent pathway for antigen-presenting cells 4). Their simultaneous progression contributes to the loss of immune privilege and rejection in corneal transplantation 4). VEGF-A/VEGFR-2 primarily drives angiogenesis, while VEGF-C,D/VEGFR-3 mainly drives lymphangiogenesis 4).
7. Latest research and future perspectives
Section titled “7. Latest research and future perspectives”Gene therapy using AAV vectors
Section titled “Gene therapy using AAV vectors”Xie et al. (2024) reviewed the treatment of corneal neovascularization through sustained anti-VEGF factor expression using adeno-associated virus (AAV) vectors 5). AAV2 and AAV8 are the most efficient for transducing corneal stromal cells, and intrastromal injection is considered the most effective route of administration 5). AAV gene therapy can provide long-term anti-VEGF effects with a single dose, but it is currently still at the preclinical stage 5).
Intravascular Mitomycin C Chemoembolization (MICE)
Section titled “Intravascular Mitomycin C Chemoembolization (MICE)”Addeen et al. (2023) reported two cases of MICE (intravascular injection of MMC 0.4 mg/mL using a 33-gauge needle) for refractory corneal neovascularization after corneal transplantation 6). Ghost vessels were observed early postoperatively, with pain reduction and improved quality of life 6). No adverse events were noted, but long-term safety needs to be confirmed.
Antisense Oligonucleotide (Aganirsen)
Section titled “Antisense Oligonucleotide (Aganirsen)”In a 2026 review by Muller et al., the antisense oligonucleotide Aganirsen, targeting IRS-1, was reported to induce regression and remission of corneal neovascularization in preclinical models1). CRISPR/Cas9-mediated editing of VEGF-A has also shown promising preclinical data1).
Ocular Nanosystems
Section titled “Ocular Nanosystems”Zhang et al. (2022) reported that nanocarriers such as nanoparticles, liposomes, and micelles can improve the corneal delivery efficiency of anti-VEGF drugs and steroids, enabling sustained release, targeted delivery, and reduced irritation7). Clinical application is still limited, but they are expected to reduce the burden of frequent dosing.
Importance of Combination Therapy
Section titled “Importance of Combination Therapy”Corneal neovascularization is a multifactorial condition, so monotherapy often fails to achieve sufficient efficacy 1)2). Combination therapy targeting multiple pathways such as VEGF, bFGF, PDGF, and lymphangiogenesis may become the cornerstone of future treatment strategies 1).
8. References
Section titled “8. References”- Muller E, Feinberg L, Woronkowicz M, Roberts HW. Corneal Neovascularization: Pathogenesis, Current Insights and Future Strategies. Biology. 2026;15(2). doi:10.3390/biology15020136. PMID:41594872; PMCID:PMC12837649.
- Wu D, Chan KE, Lim BXH, Lim DK, Wong WM, Chai C, et al. Management of corneal neovascularization: Current and emerging therapeutic approaches. Indian journal of ophthalmology. 2024;72(Suppl 3):S354-S371. doi:10.4103/IJO.IJO_3043_23. PMID:38648452; PMCID:PMC467007.
- Drzyzga Ł, Śpiewak D, Dorecka M, Wyględowska-Promieńska D. Available Therapeutic Options for Corneal Neovascularization: A Review. International journal of molecular sciences. 2024;25(10). doi:10.3390/ijms25105479. PMID:38791518; PMCID:PMC11121997.
- Zhang Z, Zhao R, Wu X, Ma Y, He Y. Research progress on the correlation between corneal neovascularization and lymphangiogenesis (Review). Molecular medicine reports. 2025;31(2). doi:10.3892/mmr.2024.13412. PMID:39635819; PMCID:PMC11638739.
- Xie M, Wang L, Deng Y, et al. Sustained and Efficient Delivery of Antivascular Endothelial Growth Factor by AAV for Treatment of Corneal Neovascularization. J Ophthalmol. 2024;2024:5487973.
- Addeen SZ, Oyoun Z, Alfhaily H, Anbari A. Outcomes of mitomycin C intravascular chemoembolization (MICE) in refractory corneal neovascularization after failed keratoplasty. Digital journal of ophthalmology : DJO. 2023;29(1):9-13. doi:10.5693/djo.02.2023.01.002. PMID:37101562; PMCID:PMC10125729.
- Zhang C, Yin Y, Zhao J, Li Y, Wang Y, Zhang Z, et al. An Update on Novel Ocular Nanosystems with Possible Benefits in the Treatment of Corneal Neovascularization. International journal of nanomedicine. 2022;17:4911-4931. doi:10.2147/IJN.S375570. PMID:36267540; PMCID:PMC9578304.