Corneal leukoma is a scar-like white opacity that occurs in the corneal stroma. It is an irreversible opacity that remains after the active phase of various keratitis, trauma, or inflammation has subsided, characterized by a hard texture without edema or infiltration.
Corneal scars are classified into three grades based on severity.
Nubecula
A faint, cloud-like opacity.
It is difficult to see with the naked eye and may only be recognized under a slit-lamp microscope.
Often only mildly affects vision.
Macula
Moderate localized opacity.
Details of the iris become difficult to see through.
If it involves the pupillary area, it can cause decreased vision.
Leukoma
Dense white opaque opacity.
The iris and pupil become invisible.
If in the pupillary area, it causes severe visual impairment.
Since the cornea is a transparent tissue, even a small scar directly reduces optical function. Even mild scar opacity can significantly reduce visual function due to irregular astigmatism.
QDoes corneal leukoma heal on its own?
A
Corneal leukoma is a scar of the corneal stroma and in principle does not resolve spontaneously. However, mild opacity (nebula level) may improve to some extent as inflammation subsides. If the leukoma involves the pupillary area, it significantly affects vision, so consult an ophthalmologist.
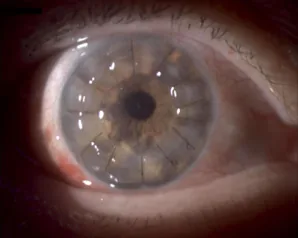
Alina Gabriela Gheorghe, Ana Maria Arghirescu, Andrei Coleașă, Ancuța Georgiana Onofrei The surgical management of a patient with Fuchs endothelial dystrophy and cataracts 2024 Jan-Mar Rom J Ophthalmol. 2024 Jan-Mar; 68(1):75-80 Figure 1. PMCID: PMC11007553. License: CC BY.
Clinical photograph showing the state one month after corneal transplant surgery in the right eye. In the central cornea, sutures for the transplanted cornea are visible.
Infectious keratitis is one of the most common causes of corneal leukoma.
Bacterial keratitis: Streptococcus pneumoniae can cause serpiginous corneal ulcer after eye exposure1). Pseudomonas aeruginosa leads to severe ulcer with ring abscess and can rapidly progress to perforation1). Gram-positive cocci form round, localized abscesses, while gram-negative rods tend to form ring abscesses1).
Fungal keratitis: Plant-related trauma and long-term use of steroid eye drops are risk factors1). Filamentous fungi present with gray-white ulcers with feathery margins (hyphate ulcer), and endothelial plaque on the posterior corneal surface is characteristic1).
Viral keratitis: HSV and varicella-zoster virus cause immunologic corneal stromal infiltration. It progresses through geographic keratitis and disciform keratitis to scarring.
Acanthamoeba keratitis: Common in contact lens wearers1). Early radial keratoneuritis progresses to ring infiltration and leaves scars.
Penetrating trauma: Scarring occurs during the wound healing process of the corneal stroma.
Chemical trauma: Alkali penetrates deep into the corneal stroma and tends to cause extensive scarring.
Birth trauma (during passage through birth canal): Forceps delivery, etc., can apply external force to the cornea, causing Descemet’s membrane rupture leading to corneal edema, and after several weeks to months, vertical linear opacities and high astigmatism remain.
Stevens-Johnson syndrome / Toxic epidermal necrolysis: In the acute phase, extensive keratoconjunctival epithelial defects occur. If corneal epithelial stem cells are lost, conjunctival tissue with connective tissue and blood vessels covers the cornea, causing severe opacity.
Ocular cicatricial pemphigoid: Symblepharon and conjunctival invasion progress gradually, leading to corneal opacity. Surgical intervention carries a risk of rapid deterioration.
Granular corneal dystrophy (type I and II): Caused by mutations in the TGFBI gene. Granular opacities increase with age; type II (Avellino type) causes diffuse opacities in the superficial cornea.
Lattice corneal dystrophy: Amyloid deposits cause linear or lattice-like opacities. In type 1, central opacities are more prominent.
Macular corneal dystrophy: Autosomal recessive inheritance. Diffuse ground-glass opacities spread throughout the entire corneal stroma, and vision loss is usually noticed between ages 10 and 30.
Fuchs endothelial corneal dystrophy: Degeneration of corneal endothelial cells leads to bullous keratopathy3). It tends to develop in middle-aged and older individuals, with a higher prevalence in women 3).
Cases of diffuse white granular opacities from the subepithelium to the stroma have been reported after long-term oral administration of atovaquone 4). Lipophilic drugs such as amiodarone and chloroquine can also cause corneal deposits due to their cationic amphiphilic structure 4).
QCan using contact lenses cause corneal leukoma?
A
Improper use of contact lenses is a risk factor for bacterial keratitis and Acanthamoeba keratitis. If these infections become severe, they can leave corneal scars (leukoma). Regular replacement of lens cases, correct use of disinfecting solutions, and adherence to wearing time are important for prevention.
This is the basic method for evaluating corneal opacities. The location (central, paracentral, peripheral), depth (subepithelial, superficial stromal, deep stromal), extent, and density of the opacity are observed. Fluorescein staining is used to check for epithelial defects.
In the differential diagnosis of corneal opacities, it is important to distinguish between infiltrative opacities due to infectious keratitis and scarred opacities. Infiltrative lesions are accompanied by surrounding edema and anterior chamber inflammation, suggesting activity 1). Ring infiltrates can be seen in both fungal keratitis and Acanthamoeba keratitis, but radial corneal neuritis and severe pain are characteristic of Acanthamoeba 2).
This allows objective evaluation of the depth of corneal lesions 1). Findings such as increased or decreased corneal thickness, anterior chamber inflammatory cells, keratic precipitates (KP), and endothelial plaque can also be observed. Treatment efficacy can be assessed by comparing before and after treatment.
This is useful for evaluating irregular astigmatism1). Even if the opacity due to corneal leukoma is mild, visual function may be significantly reduced due to irregular astigmatism.
This allows non-invasive observation of cells, nerve fibers, and microorganisms (fungal hyphae, Acanthamoeba cysts) within the cornea1). It is also useful for evaluating the cellular composition of scar tissue, but requires skill to perform and interpret the results.
This is performed when active infectious keratitis is suspected 1). Gram staining is used to estimate the causative organism, and culture on blood agar and chocolate agar is used for definitive diagnosis.
No. Corneal leukoma is an opacity of the cornea (the transparent membrane at the front of the eye), while cataract is an opacity of the lens (the lens behind the cornea). Both can cause vision loss, but their pathology and treatment differ. They can be easily distinguished with a slit-lamp microscope.
If the underlying disease causing corneal leukoma is still active, treatment of the cause is prioritized first.
Infectious keratitis: Frequent instillation of antibacterial agents (fluoroquinolones, cephalosporins, aminoglycosides) according to the causative bacteria is the basic treatment1). For fungal infections, antifungal agents are used; for viral infections, antiviral agents are used.
Inflammatory diseases: Anti-inflammatory treatment with steroid eye drops and immunosuppressive agents.
Glasses and contact lenses: For mild opacities or irregular astigmatism, correction with hard contact lenses may be possible.
Scleral lenses and PROSE devices: For corneal opacity and neovascularization associated with Stevens-Johnson syndrome/toxic epidermal necrolysis, wearing a PROSE device has been reported to induce regression of corneal opacity and neovascularization7). The back channel design of the device promotes tear exchange and improves the ocular surface environment7).
Therapeutic laser keratectomy: First choice for opacities confined to the superficial corneal layer. Effective for superficial opacities in granular corneal dystrophy type I and Avellino type. Usually can be performed up to about two times.
Corneal endothelial transplantation (DSAEK/DMEK): Performed for opacities due to endothelial diseases such as Fuchs endothelial corneal dystrophy3). First choice if stromal changes are minimal.
Artificial cornea (keratoprosthesis): For severe cases where conventional corneal transplantation is difficult (e.g., Stevens-Johnson syndrome/toxic epidermal necrolysis, ocular cicatricial pemphigoid), artificial corneas such as the Boston KPro are considered.
Corneal transparency is maintained by the regular lattice arrangement of collagen fibers in the corneal stroma. Scar formation after corneal injury follows the following process.
Apoptosis of keratocytes: Following epithelial damage due to trauma or infection, keratocytes at the injury site undergo apoptosis.
Differentiation into myofibroblasts: TGF-β1 and TGF-β2 released from tears and epithelium infiltrate the corneal stroma and differentiate surviving keratocytes into myofibroblasts5).
Production of abnormal extracellular matrix: Myofibroblasts produce disorganized collagen and extracellular matrix, leading to loss of transparency5).
Damage to the epithelial basement membrane (EBM): Normal EBM controls the inflow of TGF-β into the stroma, but when this barrier is disrupted by injury, fibrosis persists5).
Corneal stromal opacities are classified into the following three types.
Inflammatory opacity (infiltrative lesion): Active infectious foci such as bacterial or fungal keratitis. Caused by accumulation of neutrophils and lymphocytes. When an abscess forms, tissue destruction progresses due to proteolytic enzymes, leaving a scar with thinning after healing1).
Edematous opacity: Increased water content in the stroma due to corneal endothelial dysfunction. In Fuchs endothelial corneal dystrophy, degenerated endothelial cells protrude abnormal collagen-like material on the posterior surface of Descemet’s membrane (guttae), and as the disease progresses, the pump and barrier functions of the endothelium decline, leading to bullous keratopathy3).
Depositional opacity: Deposition of substances due to corneal dystrophies (granular, lattice, macular) or metabolic diseases. In macular corneal dystrophy, CHST6 gene mutation impairs sulfation of keratan sulfate, and hyposulfated keratan sulfate accumulates diffusely inside and outside corneal stromal cells.
Drugs with a cationic amphiphilic structure, such as atovaquone, consist of a hydrophobic ring and a hydrophilic cationic amine side chain, and they cross cell membranes to cause accumulation of phospholipids4). Amiodarone reaches the cornea via tears, aqueous humor, and limbal vessels, and drug-lipid complexes form within lysosomes4).
Dutra et al. (2025) reported three cases of corneal scarring due to HSV or varicella-zoster virus keratitis treated with 0.8 mg/mL losartan eye drops administered six times daily 5). In a 40-year-old woman with HSV scarring (Case 1), BCVA improved from 20/60 to 20/25 after 16 weeks of treatment, and AS-OCT confirmed regression of stromal opacity. In a 15-year-old male with varicella-zoster virus scarring (Case 3), BCVA improved from 20/200 to 20/20 5).
Losartan is an angiotensin II receptor antagonist that induces apoptosis of myofibroblasts by inhibiting the non-canonical pathway of TGF-β (ERK-mediated signaling) 5). After removal of myofibroblasts, corneal fibroblasts repopulate, leading to regeneration of the epithelial basement membrane and absorption/reorganization of disorganized collagen, thereby restoring transparency 5). Treatment effects may take 6 to 9 months to manifest 5).
Long-term Effects of PROSE Device for Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis
Liao et al. (2022) reported regression of corneal opacity and neovascularization in two cases (four eyes) of Stevens-Johnson syndrome/toxic epidermal necrolysis with continuous wear of a back-channel designed PROSE device 7). In Case 1 (19-year-old female with Stevens-Johnson syndrome), corneal opacity in the left eye improved from grade 1 to 0, and BCVA improved from 20/40 to 20/15. In Case 2 (26-year-old male with toxic epidermal necrolysis), all prescribed eye drops were discontinued after 17 months of PROSE wear, with sustained improvement in corneal neovascularization and opacity 7).
Ashizuka et al. (2025) reported a 15-year-old male who developed bilateral diffuse corneal stromal opacity after 14 months of oral atovaquone for aplastic anemia 4). Anterior segment OCT showed uniform diffuse opacity without changes in corneal shape, and in vivo confocal microscopy confirmed pigment deposition in the corneal stroma. Corneal opacity persisted one year after discontinuation of atovaquone 4).
Megalla et al. (2021) reported a case of bilateral symmetric annular corneal stromal opacity (Ascher ring) in a 70-year-old male 6). Ascher ring is an extremely rare idiopathic stromal opacity first described in 1964, characterized by bilaterality and no effect on visual function 6). No genetic pattern or laboratory abnormalities have been identified, and it is diagnosed by exclusion 6).
Rhee MK, Ahmad S, Amescua G, et al.; American Academy of Ophthalmology Preferred Practice Pattern Cornea/External Disease Panel. Bacterial Keratitis Preferred Practice Pattern®. Ophthalmology. 2024;131(4):P87-P133. PMID: 38349295. doi:10.1016/j.ophtha.2023.12.035.
Matthaei M, Hribek A, Clahsen T, Bachmann B, Cursiefen C, Jun AS. Fuchs Endothelial Corneal Dystrophy: Clinical, Genetic, Pathophysiologic, and Therapeutic Aspects. Annual review of vision science. 2019;5:151-175. doi:10.1146/annurev-vision-091718-014852. PMID:31525145. PMID: 31525145. doi:10.1146/annurev-vision-091718-014852.
Ashizuka T, Uematsu M, Mohamed MT, Kusano M, Helmy MY, Inoue D, et al. A case of corneal opacity caused by atovaquone administration. American journal of ophthalmology case reports. 2025;37:102235. doi:10.1016/j.ajoc.2024.102235. PMID:39803603; PMCID:PMC11720875.
Dutra BAL, Drew-Bear LE, Herretes SP, Arroyo D, de Oliveira RC, Sampaio LP, et al. Topical Losartan Treatment of Herpes Simplex Virus- or Varicella-Zoster Virus-Induced Corneal Scarring: A Case Series. Case reports in ophthalmology. 2025;16(1):281-289. doi:10.1159/000545215. PMID:40248823; PMCID:PMC12005691.
Megalla M, Li E, Branden P, Chow J. Bilateral idiopathic corneal opacity: A report of Ascher ring and a review of the literature. Am J Ophthalmol Case Rep. 2021;23:101176.
Liao J, Asghari B, Carrasquillo KG. Regression of corneal opacity and neovascularization in Stevens-Johnson syndrome and Toxic Epidermal Necrolysis with the use of prosthetic replacement of the ocular surface ecosystem (PROSE) treatment. Am J Ophthalmol Case Rep. 2022;26:101520.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.