Corneal topography is a non-invasive, quantitative imaging technique that measures and visualizes the shape of the anterior corneal surface. The earliest topography is attributed to Scheiner’s studies using corneal reflections in the early 17th century, and significant progress was made with the introduction of the Placido disc in the late 19th century.
Corneal tomography is an advanced technique that measures the three-dimensional structure including the shape of both the anterior and posterior corneal surfaces and the distribution of corneal thickness1). Clinically, topography and tomography are combined for comprehensive corneal evaluation.
Corneal Topography
Measurement target: Shape of the anterior corneal surface
Principle: Mainly Placido ring reflection
Data provided: Corneal power map (curvature)
Advantages: High reproducibility and spatial resolution. Suitable for normal to moderate irregular astigmatism.
Corneal Tomography
Measurement target: Three-dimensional structure of anterior and posterior corneal surfaces
Data provided: Maps of anterior and posterior curvature, elevation, and corneal thickness
Advantages: Allows evaluation of the posterior corneal surface. May be measurable even in the presence of opacity or edema1)
QWhat is the difference between topography and tomography?
A
Topography is a technique that primarily uses Placido ring reflections to measure the shape (curvature) of the anterior corneal surface. Tomography, on the other hand, uses Scheimpflug cameras or anterior segment OCT to measure the three-dimensional structure of the cornea, including the anterior and posterior surfaces and thickness. In conditions such as keratoconus, changes in the posterior surface may appear before those in the anterior surface, making tomographic evaluation more important.
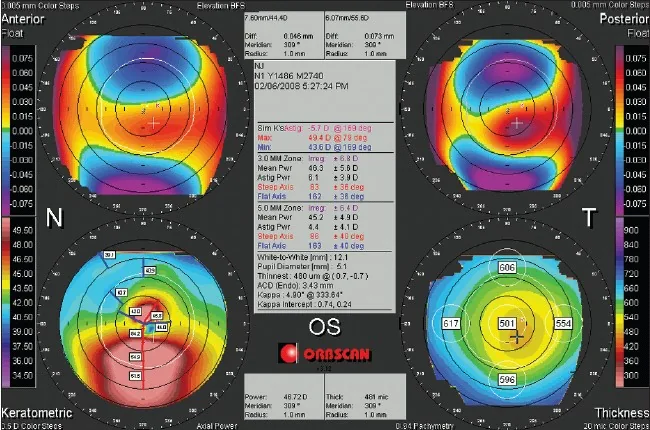
Hassan Hashemi, Shiva Mehravaran Day to Day Clinically Relevant Corneal Elevation, Thickness, and Curvature Parameters Using the Orbscan II Scanning Slit Topographer and the Pentacam Scheimpflug Imaging Device 2010 Jan-Mar Middle East Afr J Ophthalmol. 2010 Jan-Mar; 17(1):44-55 Figure 3. PMCID: PMC2880373. License: CC BY.
Orbscan quad map showing four parameters simultaneously: anterior elevation, posterior elevation, corneal power, and corneal thickness. The central numerical panel also provides information on the thinnest point and power distribution.
The main clinical indications for corneal topography and tomography are listed below.
Screening and follow-up of keratoconus: Corneal topography is the gold standard for early screening of suspected keratoconus6). Early keratoconus often appears normal on slit-lamp examination, and topography may be the only clue. Typical patterns include inferior steepening (I-S ratio ≥1.2) and skewing of the radial axis >21°6). In children and young adults, progression on tomography has been confirmed in 77% of eyes7), making regular follow-up important. Atypical cases such as temporal keratoconus have also been reported3). In a 14-year-old case, Pentacam detected temporal steepening and thinning, and the T-N (temporal-nasal) ratio was useful for diagnosis instead of the I-S ratio3).
Planning and postoperative evaluation of refractive surgery: In determining the indication for refractive surgery, excluding potential corneal ectasia is essential6). Postoperatively, it is used to evaluate dioptric changes in the cornea and to detect decentered ablation or ablation failure. In topography-guided LASIK (e.g., CONTOURA), anterior corneal surface data acquired with the Topolyzer Vario directly determine the laser ablation pattern2).
Evaluation of corneal surface irregularity: Placido ring mires are useful for assessing irregular astigmatism due to subepithelial infiltrates after adenoviral conjunctivitis. Fine surface irregularities that are difficult to detect on SS-OCT color maps can be visualized as ring distortions4).
Other indications: Also used for astigmatism evaluation after cataract surgery and corneal transplantation, contact lens fitting, and assessment of corneal shape changes due to pterygium or corneal opacity.
Concentric rings (Placido disc) are projected onto the tear film on the anterior corneal surface, and the corneal curvature is calculated from the shape of the reflected image. There are large cone types (TMS, Atlas, etc.) and small cone types (Keratograph, etc.), and color LED methods (Cassini) have also emerged1).
Advantages: High spatial resolution and reproducibility. Optimal for measuring the anterior corneal surface.
Limitations: Affected by tear film instability. The posterior corneal surface cannot be measured. Only about 60% of the corneal surface is evaluated, limiting detection of peripheral lesions (e.g., pellucid marginal degeneration)6).
Placido ring mires can qualitatively assess corneal irregularity without a device, and are particularly useful in pediatric or uncooperative patients4).
Scheimpflug images are captured using a rotating slit light to reconstruct the three-dimensional structure of the anterior and posterior corneal surfaces1). Representative devices include Pentacam (single rotating Scheimpflug), Galilei (dual Scheimpflug + Placido), and Sirius (Scheimpflug + Placido)1).
Advantages: Simultaneously obtains curvature, elevation, and corneal thickness maps of both anterior and posterior surfaces.
Limitations: Cannot observe tissues that do not transmit light. The angle is difficult to image due to oblique incidence of illumination light. There are issues with correction accuracy due to refractive surface effects.
Three-dimensional corneal structure is reconstructed from OCT cross-sectional images 1). SS-OCT (wavelength 1,310 nm, CASIA, etc.) has a wide measurement range and can depict the entire cornea in a single image. SD-OCT (wavelength 840 nm) has a narrower measurement range but achieves high resolution.
Advantages: Corneal shape analysis is possible even with opacity or edema. Non-contact and fast. Less affected by the tear film. Can be taken in dark conditions.
The Belin-Ambrosio enhanced ectasia display is a function on the Pentacam that integrates and displays the spatial profile of corneal thickness and deviations in anterior and posterior elevation, improving screening accuracy for corneal ectasia5).
5. Examination Technique and Interpretation of Results
Fix the patient’s head on the chin rest and forehead strap, and have them gaze at the fixation light. Align focus and centering, then capture the image. Be careful of poor fixation, inadvertent eye compression, and corneal deformation due to eyelid elevation. Take at least two images to confirm reproducibility. For contact lens users, a discontinuation period of two weeks or more is recommended 6).
Power maps (axial / tangential / refractive): Display corneal refractive power in color code. Axial power is based on slope and is robust to noise. Tangential (instantaneous) power reflects local curvature and is excellent for identifying the apex of keratoconus. Refractive power reflects optical properties based on Snell’s law.
Elevation maps: Display the difference between the corneal surface and a reference sphere as height. Isolated elevations on the anterior and posterior surfaces are important indicators of corneal ectasia6). Posterior elevation maps show high sensitivity and specificity for detecting forme fruste keratoconus6).
Pachymetry maps: Display corneal thickness distribution. In a normal cornea, the center is thinnest and gradually increases toward the periphery. Eccentricity of the thinnest point suggests corneal ectasia.
Correlate with slit-lamp findings. Be aware of artifacts due to corneal scars, dry eye, and neovascularization
QHow long is the required contact lens discontinuation period?
A
Contact lenses (especially rigid gas permeable lenses) temporarily alter corneal shape, so a discontinuation period is necessary to obtain accurate topography data. Generally, at least 2 weeks for soft lenses and a longer period (2–4 weeks) for rigid lenses is recommended. Strict discontinuation is particularly required in important situations such as evaluating candidacy for refractive surgery.
6. Optical Principles and Detailed Measurement Principles
There are three definitions of corneal power used in corneal topography.
Axial power (sagittal power): Pa = (n-1)/d. Calculated from the distance d from the normal line at the measurement point to the reference axis. It is robust to noise based on slope. It extends keratometer-like measurements to a wide area.
Instantaneous power (tangential power): Pi = (n-1)/r. Calculated from the local radius of curvature r at the measurement point. It reflects local shape changes more accurately but is sensitive to noise.
Refractive power (focal power): Pr = n/f. Based on the focal length f. It most accurately reflects optical properties based on Snell’s law.
Autokeratometers and Placido-based devices measure only the anterior corneal surface and do not consider the posterior surface. Assuming that the shapes of the anterior and posterior surfaces are proportional, the keratometric index (usually 1.3375) is used instead of the refractive index of the corneal stroma to calculate total corneal power. This assumption generally holds for normal corneas, but after refractive surgery or in corneal ectasia, the proportional relationship between the anterior and posterior surfaces is disrupted, leading to errors 1).
In ideal photography, the lens plane and image plane are parallel, but for non-planar objects like the cornea, image distortion occurs. According to the Scheimpflug principle, by adjusting the image plane and lens plane so that the extensions of the object plane, lens plane, and image plane intersect at a single point (Scheimpflug intersection), a focused image can be obtained even for non-planar objects 1). This principle enables distortion-free imaging of slit-light corneal cross-sections.
Combining corneal shape analysis with wavefront aberration analysis allows quantitative evaluation of spherical and cylindrical components (second-order aberrations) as well as higher-order aberrations (coma, spherical aberration, etc.). Aberrations are expanded using Zernike polynomials and quantified as RMS (root mean square) values. In keratoconus, a marked increase in vertical coma aberration is characteristic 6). Some devices can perform topography and aberration analysis simultaneously 1).
In recent years, combined devices that integrate topography, tomography, and biometric measurements (axial length, anterior chamber depth, etc.) have emerged 1). The concept of Total Corneal Refractive Power for intraocular lens power calculation has been proposed, and it is expected to improve the accuracy of power calculation in cataract surgery, especially after refractive surgery 1).
Custom ablation based on topography data is widely used in refractive surgery. The anterior corneal surface data obtained with the Topolyzer Vario directly determines the laser ablation pattern for CONTOURA surgery 2). A 3Z nomogram has been proposed to address discrepancies between subjective refractionastigmatism values and topographic astigmatism values 2). Combined PTK and topography-guided PRK for corneal scars has also been reported.
The Belin-Ambrosio enhanced ectasia display integrates corneal thickness spatial profile (CTSP) and percentage thickness increase (PTI), improving detection accuracy for subclinical keratoconus5). The tomographic and biomechanical index (TBI) combined with Corvis ST enables comprehensive screening that also considers corneal biomechanics5). Reports of atypical cases such as temporal keratoconus3) suggest the importance of multi-angle evaluation including the T-N ratio, not just the standard I-S ratio.
In evaluating irregular astigmatism due to subepithelial infiltrates (SEI) after adenovirus infection, it has been reported that Placido ring mires can detect surface irregularities more sensitively than SS-OCT color maps 4). Serial Placido ring imaging was also useful for monitoring treatment with tacrolimus eye drops 4). Even in settings where advanced equipment is not available, qualitative assessment of Placido ring images can be a simple and effective screening tool for corneal surface abnormalities.
QCan corneal topography help in early detection of keratoconus?
A
Yes, corneal topography is the gold standard for early screening of keratoconus. Even in early keratoconus where slit-lamp examination appears normal, topography can detect characteristic patterns such as inferior steepening. Furthermore, combining tomography (e.g., Pentacam) allows evaluation of posterior corneal changes and comprehensive assessment using the Belin-Ambrosio display, enabling earlier detection.
Kanclerz P, Khoramnia R, Wang X. Current Developments in Corneal Topography and Tomography. Diagnostics (Basel, Switzerland). 2021;11(8). doi:10.3390/diagnostics11081466. PMID:34441401; PMCID:PMC8392046.
Khamar P, Shetty R, Annavajjhala S, Narasimhan R, Kumari S, Sathe P, et al. Impact of crossplay between ocular aberrations and depth of focus in topo-guided laser-assisted in situ keratomileusis outcomes. Indian journal of ophthalmology. 2023;71(2):467-475. doi:10.4103/ijo.IJO_191_22. PMID:36727342; PMCID:PMC10228944.
Zhang LJ, Traish AS, Dohlman TH. Temporal keratoconus in a pediatric patient. American journal of ophthalmology case reports. 2023;32:101900. doi:10.1016/j.ajoc.2023.101900. PMID:37546376; PMCID:PMC10400863.
Toyokawa N, Araki-Sasaki K, Kimura H, Kuroda S. Evaluating anterior corneal surface using Placido ring mires for irregular astigmatism in refractory corneal subepithelial infiltrates after adenoviral conjunctivitis. BMC ophthalmology. 2024;24(1):515. doi:10.1186/s12886-024-03774-2. PMID:39609742; PMCID:PMC11603996.
Nelapatla GI, Chaurasia S. Pellucid marginal corneal degeneration in a teenager. BMJ Case Rep. 2022;15:e248599.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Meyer JJ, Gokul A, Vellara HR, McGhee CNJ. Progression of keratoconus in children and adolescents. The British journal of ophthalmology. 2023;107(2):176-180. doi:10.1136/bjophthalmol-2020-316481. PMID:34479856.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.