Pellucid marginal corneal degeneration (PMD, PMCD) is a non-inflammatory, non-hereditary corneal ectasia characterized by bilateral inferior peripheral corneal thinning. The term “pellucid” means “transparent,” referring to the clear appearance of the thinned area. There are no inflammatory findings such as vascular invasion or opacification in the thinned area, and it is considered a related disease to keratoconus.
PMD is the second most common non-inflammatory corneal thinning disease after keratoconus. However, it is often misdiagnosed as keratoconus, so the actual prevalence may be underestimated 3). PMD typically develops in the 30s to 50s 2,4), slightly later than keratoconus, and is more common in males.
Since PMD shares many clinical and histological features with keratoconus, some view keratoconus and PMD as a continuous spectrum 3). About 10% of PMD cases are complicated by keratoconus and about 13% by keratoglobus4). Cases of coexisting PMD and keratoconus in the same patient have been reported; a Japanese nationwide survey found that among 27 unilateral PMD cases, 17 had keratoconus or suspected keratoconus in the contralateral eye 1).
Progression of corneal shape abnormalities leads to severe irregular astigmatism and visual impairment. There is a strong tendency toward against-the-rule astigmatism, and correction with glasses or contact lenses is often more difficult than in keratoconus4).
PMD often has a long asymptomatic period; it is frequently missed during health checkups or eyeglass prescriptions in the 20s, and is first diagnosed in the 30s to 40s when against-the-rule astigmatism increases and corrected visual acuity becomes inadequate. In contrast to keratoconus, which is detected relatively early due to acute hydrops or marked central corneal protrusion, PMD progresses slowly as “untreatable against-the-rule astigmatism” or “gradually ill-fitting glasses.” Epidemiological data are limited, and no large-scale national studies like those for keratoconus have been conducted, so the true prevalence is unknown. Cases are also reported where PMD is incidentally discovered during preoperative examinations for refractive surgery, suggesting that the number of potential patients is not small.
QWhat is the difference from keratoconus?
A
In PMD, the lower peripheral cornea becomes thin, and the maximum protrusion is located above (centrally) the thin area. In keratoconus, the central to paracentral cornea becomes thin, and the thin area coincides with the protrusion. PMD does not show Fleischer rings or Vogt striae, and tends to have high against-the-rule astigmatism. PMD often develops after the 30s, whereas keratoconus develops in adolescence.
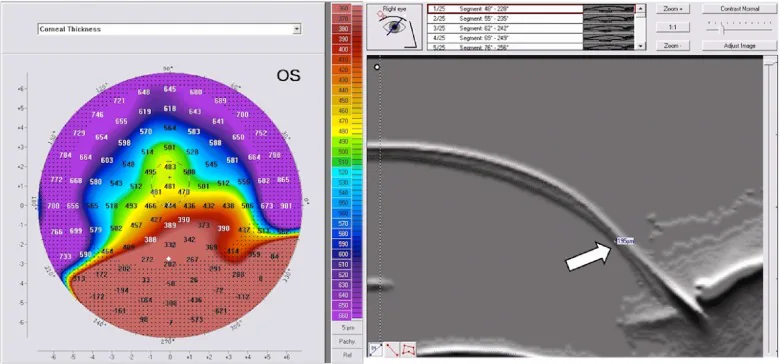
Sinjab MM, et al. Pellucid-like keratoconus. F1000Res. 2012. Figure 2. PMCID: PMC3752625. License: CC BY.
Inferior corneal thinning measured by corneal thickness in PMD: A shows the Bell sign on the thickness map, and B shows the thinning site on the Scheimpflug image (white arrow). This corresponds to the inferior corneal thinning discussed in the section “2. Main Symptoms and Clinical Findings.”
From 4 to 8 o’clock, 1–2 mm from the limbus, width 1–2 mm
Anterior protrusion
Located above (centrally) the thin area, beer belly-like appearance
Corneal transparency
Thinned area is transparent, no vascular invasion or opacity
Epithelium
Always preserved (no lipid deposition)
Thinning is present 1–2 mm above the limbus, in a band 1–2 mm wide, extending from the 4 to 8 o’clock direction. It may thin to 20% of normal corneal thickness. The area of maximal protrusion is located above the thinned area, and the corneal cross-section appears like a “beer belly” 2). This protrusion causes high against-the-rule astigmatism of up to 20 D, making visual correction extremely difficult.
In PMD, Fleischer ring, cone (apex), and apical scarring are absent. The cornea between the thinned area and the limbus is healthy, and the thinned area is always epithelialized. It is distinguished from Terrien marginal degeneration by the absence of lipid deposition.
Crab claw pattern: A characteristic finding of crescent-shaped steepening in the inferior cornea on the corneal power map
Butterfly pattern: A vertical, cool-colored butterfly-shaped pattern in the central area
Kissing doves / kissing birds pattern: Appearance seen on Scheimpflug imaging 5)
Against-the-rule astigmatism and large radius of curvature: Keratometry shows strong against-the-rule astigmatism, but unlike keratoconus, the corneal curvature radius tends to be larger
However, crab claw-like findings can also be seen in advanced keratoconus and are not specific to PMD 3). Corneal elevation maps show protrusion in the inferior periphery on both anterior and posterior surfaces, and the thinnest point on the corneal thickness map is located slightly inferior to the protrusion.
Placido-based corneal topography can evaluate only about 60% of the corneal surface, limiting its assessment of PMD, a peripheral disease 2). Scheimpflug imaging or slit-scanning tomography (Pentacam, Orbscan, etc.) can evaluate the anterior and posterior corneal surfaces and the full pachymetry map, and are useful for diagnosing PMD and differentiating it from keratoconus2,5). In particular, bulging of the posterior elevation into the inferior periphery and the finding that the thinnest point is located inferior to the protrusion are important elements contributing to the diagnosis of PMD. Distinguishing PMD from keratoconus is clinically important, but transitional cases exist, making it difficult to confirm based solely on imaging findings; longitudinal observation of progression is required.
The ABCD classification integrated into Scheimpflug imaging is used to assess progression of corneal ectasia. It is a composite score consisting of four elements: anterior radius of curvature (A), posterior radius of curvature (B), minimum corneal thickness (C), and best spectacle-corrected distance acuity (D), and is used to track changes over time 2).
The etiology of PMD is not clear, but it is thought that thinning and protrusion occur due to a combination of weakening caused by structural abnormalities of corneal stromal collagen and mechanical stress from intraocular pressure. Histologically, the stromal collagen shows fibrous long-spacing (FLS) collagen with a period of 100–110 nm, which differs from the normal collagen period of 60–64 nm. This structural abnormality may contribute to corneal weakening 4).
In recent years, there has been discussion about considering PMD and keratoconus as diseases on the same spectrum. Belin et al. have proposed that “pellucid marginal degeneration is not an independent disease but should be considered a phenotype of inferiorly displaced keratoconus” 3). This view is based on numerous reports of coexisting PMD and keratoconus in the same patient, common histological and collagen abnormalities, and continuity in imaging findings. On the other hand, in clinical practice, it is still common to treat PMD as an independent phenotype due to differences in thinning site, protrusion site, age of onset, and progression rate.
Allergic predisposition: Allergic conditions such as atopic dermatitis and asthma are present in about 30% of patients. A national survey in Japan reported allergic predisposition in 22.2% of cases 1).
Eye rubbing: It is suggested to be a factor that exacerbates corneal ectasia, and allergy control with mast cell stabilizers is recommended 2).
Allergy and perforation risk: Allergic predisposition is considered a risk factor for acute hydrops and corneal perforation 1,2). Ueji et al. reported that among 18 cases of corneal perforation due to PMD, 6 had allergic predisposition or a habit of eye rubbing 1).
Obstructive sleep apnea syndrome and high BMI: An association with corneal ectasia in general has been reported 2).
Genetic factors: PMD alone is considered non-hereditary, but in recent years, associations with corneal collagen-related genes such as KERA gene mutations have been reported.
QDoes allergy worsen PMD?
A
Allergic predisposition is considered a risk factor for acute hydrops and corneal perforation. In keratoconus, allergic predisposition is known as a risk factor for acute hydrops, and a similar association is suggested in PMD. Ocular itching due to allergies may trigger eye rubbing, increasing mechanical stress on the cornea. Early anti-allergy treatment and addition of mast cell stabilizers may be effective in preventing perforation.
The diagnosis of PMD is based on slit-lamp examination and medical history, supported by corneal topography. The presence of a band of thinning in the inferior peripheral cornea (clear, non-inflammatory, without lipid deposition) and protrusion above the thinned area suggests PMD.
Refraction testing typically reveals high against-the-rule astigmatism and irregular astigmatism that are difficult to correct with standard spectacle prescriptions 4). Retinoscopy shows a scissors reflex 2). Mild cases are often misdiagnosed as simple against-the-rule astigmatism, so detailed corneal topography is important.
Keratometer: Detects high against-the-rule astigmatism. Unlike keratoconus, the corneal curvature radius tends to be larger.
Corneal topography (Placido-based): Detects a crab claw pattern, but has limitations in evaluating the periphery 2).
Scheimpflug tomography: Useful for diagnosis and progression assessment of PMD through anterior and posterior elevation maps and full pachymetry maps 2,5).
Slit-scanning tomography (Orbscan): Detects characteristic findings such as the kissing doves pattern.
Anterior segment OCT (AS-OCT): Evaluates pachymetry maps and epithelial thickness maps with high-resolution cross-sectional images, visualizing stromal thinning and epithelial remodeling 2).
Corneal biomechanical measurement: Decreased corneal hysteresis and corneal resistance factor are expected to be useful for early detection 2).
According to the 2015 international consensus, progression is defined as worsening in at least two of the following: steepening of the anterior corneal curvature, steepening of the posterior corneal curvature, and thinning (or increase in the rate of corneal thickness change from the periphery to the thinnest point) 2).
Thinning site: Central to paracentral cornea. PMD is inferior peripheral.
Protrusion site: Coincides with thinning. In PMD, above the thinning.
Characteristic findings: Fleischer ring, Vogt striae present. Not seen in PMD.
Age of onset: Adolescence. PMD is after 30s.
Terrien Marginal Degeneration
Inflammatory findings: Lipid deposits, pseudopterygium, superficial vascular invasion. Not seen in PMD.
Thinning pattern: More common superiorly, but can occur in any direction. PMD is inferior.
Margin shape: Shell-like, fan-shaped border.
Mooren's Ulcer
Inflammation: Severe anterior segment inflammation, presenting with corneal ulcer.
Epithelial damage: Corneal epithelial damage present. In PMD, epithelium is intact.
Simple With-the-Rule Astigmatism
Corneal thickness: No thinning observed.
Topography: Normal bow-tie pattern. No crab claw-like inferior steepening.
In preoperative evaluation for refractive surgery, if mild PMD is mistakenly diagnosed as “simple against-the-rule astigmatism” and surgery is performed, there is a risk of inducing postoperative corneal ectasia (keratectasia) 2,4). It is most important to reliably exclude PMD in preoperative screening. Especially in young patients with high against-the-rule astigmatism, unstable refraction, or findings suggesting inferior corneal thinning (inferior I/S asymmetry, elevated inferior elevation, decreased inferior pachymetry), they should be excluded from LASIK, SMILE, and PRK.
It is desirable to diagnose based on consistent findings from multiple modalities combining corneal thickness, corneal shape, and biomechanical evaluation. Since a single transient abnormal value from one test can easily lead to false positives, two or more tests tracking changes over time are recommended.
The majority of PMD cases are managed non-surgically. Reports indicate that approximately 88% are managed non-surgically, of which 36% are corrected with glasses and 52% with contact lenses 4). Glasses correction reaches its limit relatively early as against-the-rule astigmatism increases.
Lens Type
Characteristics
Rigid Gas Permeable (RGP)
Most effective for neutralizing irregular astigmatism, but prone to displacement due to inferior decentration, making fitting difficult
Scleral Lens
Does not contact the cornea, covering it for excellent stability; first choice in advanced PMD 2)
Hybrid Lens
RGP center + soft skirt. Good wearing comfort 2)
Piggyback
RGP placed over a soft CL, combining comfort and correction 2)
In PMD, because the protrusion is in the peripheral cornea, standard RGP lenses tend to shift laterally and are more difficult to fit than in keratoconus. Large-diameter RGP lenses or upper eyelid-supported lenses may be attempted, but can cause irritation or lens loss. Scleral lenses do not contact the corneal surface at all, making them effective in advanced cases or those with irregular anterior corneal shape 2). The lens and the tear film behind it function optically as a “liquid lens,” neutralizing irregular corneal astigmatism. Although it takes time to adapt to wearing them, they easily achieve both good corrected visual acuity and comfort, and in recent years they are becoming the first choice for corneal ectasias in general.
Corneal cross-linking is a treatment that forms cross-links between collagen fibers in the corneal stroma, increasing the biomechanical rigidity of the cornea to inhibit the progression of ectasia. It is approved by the US FDA for progressive keratoconus and post-corneal ectasia in patients aged 14–65 years 2), and is also applied to PMD.
Standard protocol (Dresden protocol): After removing the corneal epithelium, 0.1% riboflavin eye drops are instilled every 2 minutes for 30 minutes, then UV-A at 370 nm wavelength is irradiated at 3 mW/cm² for 30 minutes (total energy 5.4 J/cm²) 2,7)
Accelerated protocol: Methods have been developed that increase UV-A intensity to 9–30 mW/cm² and shorten irradiation time 2)
Efficacy: Cessation of ectasia progression has been reported in both early and advanced cases, along with 1.0–2.5 D of corneal flattening 2,7,8). Long-term follow-up confirms stability 10 years after CXL7)
Contraindications: Cases with corneal stromal thickness less than 400 µm at the time of UV irradiation are contraindicated due to risk of endothelial damage 2). However, individualized protocols for ultrathin corneas (sub400 protocol) have also been reported 9)
Stojanovic et al. reported the usefulness of a combined procedure of localized PRK (topography-guided transepithelial ablation) and CXL performed in one session for PMD and keratoconus6)
In the Netherlands, it has been reported that the number of corneal transplantations for keratoconus decreased by approximately 25% after the introduction of CXL10). A Cochrane review also concluded that CXL is effective in slowing the progression of corneal ectasia12). Although there are not as many large-scale RCTs for PMD as for keratoconus, multiple case reports have shown stabilization of corneal shape and flattening of maximum keratometry values. Therefore, early introduction of CXL is recommended in young to middle-aged patients with confirmed progression.
Intracorneal ring segments (ICRS, brand names: Intacs, Ferrara, etc.) are a surgical procedure in which semicircular PMMA rings are inserted into the corneal stroma to flatten the corneal shape and reduce irregular astigmatism.
Indications: Ectatic corneas with a clear center and corneal thickness of 400 µm or more 2)
Effects: Improvement in uncorrected and corrected visual acuity, reduction of higher-order aberrations, and easier contact lens fitting 2)
Technique: Femtosecond laser-assisted channel creation is the mainstream method, achieving results comparable to manual techniques 2)
Combination with CXL: Many reports add CXL after ICRS insertion to enhance the effect of slowing progression
In recent years, CAIRS (corneal allogenic intrastromal ring segments) using allogeneic corneal tissue have also been developed. In a pilot study of 24 keratoconus eyes, no segment-related complications were observed after combined CAIRS and CXL11). ICRS is primarily a means of shape change aimed at improving visual function, and its effect on slowing progression is limited. Therefore, in cases with confirmed progression, a strategy of sequential combination with CXL is adopted to obtain the benefits of both.
Surgery is considered when contact lens wear is impossible or visual correction is insufficient. In PMD, the protrusion is located in the peripheral cornea, making the procedure more complex than standard central corneal transplantation.
Peripheral crescentic lamellar keratoplasty: A procedure in which a crescent-shaped lamellar graft is inserted into the thinned area. The risk of rejection is relatively low, and it is one of the most preferred methods in recent years. If visual acuity is insufficient, a two-stage surgery with subsequent central penetrating keratoplasty is recommended.
Penetrating keratoplasty (PKP): A classic procedure. In PMD, a large graft (9.0 mm or more) must be placed eccentrically downward, which carries a higher risk of neovascularization and rejection.
Partial lamellar keratoplasty: A procedure in which the thinned area is excised in a crescent shape and replaced with a lamellar graft. If additional visual improvement is needed, a two-stage approach may be taken, with a central penetrating keratoplasty added at a later date.
Management of Acute Hydrops and Corneal Perforation
Acute hydrops is managed conservatively with hyperosmotic eye drops, intraocular pressure reduction, and gas injection, similar to keratoconus. PMD carries a risk of perforation due to the thinness of the thinned area, and management of perforated cases is clinically important.
Ueji et al. reported a case of corneal perforation due to PMD that was successfully closed with conservative treatment using a therapeutic soft contact lens (TCL), and corrected visual acuity improved to 1.0 one year postoperatively. Conservative treatment also resulted in approximately a 50% reduction in astigmatism1). A literature review of 20 eyes with corneal perforation due to PMD found that conservative treatment (tissue adhesive/TCL) was attempted in 13 eyes and was successful in 4 eyes 1). Conservative treatment is worth attempting for relatively small perforations.
QCan I undergo LASIK surgery?
A
Refractive surgery such as LASIK is contraindicated in patients with PMD. Resecting the cornea in the presence of corneal stromal thinning can induce keratectasia. Mild cases of PMD are sometimes misdiagnosed as regular against-the-rule astigmatism, so it is important to reliably exclude PMD during screening before refractive surgery.
QCan I use contact lenses?
A
Many patients with PMD can be managed with contact lenses, and approximately 88% of cases are managed non-surgically. However, due to inferior protrusion, standard hard contact lenses tend to dislodge easily, and fitting is more difficult than in keratoconus. In advanced cases, scleral lenses or hybrid lenses are often chosen. Contact lenses improve vision by neutralizing irregular astigmatism but do not slow disease progression; therefore, if progression is confirmed, corneal cross-linking (CXL) should be combined.
The histopathological findings of PMD are similar to those of keratoconus. Corneal stromal thinning is present, but the epithelium, endothelium, and Descemet’s membrane are normal. Breaks or focal disruptions of Bowman’s layer are observed, and lipid deposition is usually absent. The stromal matrix is rich in mucopolysaccharides.
Electron microscopy of the thinned area reveals abnormal fibrous long-spacing (FLS) collagen. The period of FLS collagen is 100–110 nm, significantly longer than normal collagen (60–64 nm). This FLS collagen is also observed in advanced keratoconus, supporting the relationship between the two diseases 4).
In keratoconus and related corneal ectasias, increased matrix metalloproteinase (MMP) activity and decreased endogenous inhibitors (TIMPs) have been reported, suggesting that enhanced degradation of stromal collagen contributes to thinning 2). Additionally, increases in inflammatory mediators such as IL-6, TNF-α, and MMP-9 in tears have been reported, indicating that low-grade inflammation may also play a role in PMD and keratoconus, which were traditionally considered non-inflammatory 2). These findings are consistent with clinical observations that eye rubbing and allergic stimulation exacerbate the condition. Keratocyte apoptosis induced by elevated inflammatory cytokines reduces stromal cellularity, impairing collagen fiber metabolism and remodeling, potentially leading to decreased corneal mechanical strength and thinning.
Abnormal collagen structure in the corneal stroma weakens the cornea, making it unable to withstand normal intraocular pressure, resulting in thinning and protrusion of the inferior peripheral region. The point of maximum protrusion is located above the thinnest area because, although the thinnest area is structurally weak, the stress from intraocular pressure is greatest near the boundary between the thin area and normal cornea. Due to this mechanical mechanism, the corneal cross-section exhibits a unique shape described as a “beer belly,” combining a band of thinning with upward bulging. This morphological abnormality causes severe against-the-rule astigmatism, which is a direct cause of visual impairment that cannot be adequately corrected with ordinary glasses.
When corneal thinning progresses severely, Descemet’s membrane ruptures, allowing aqueous humor to flow into the stroma, causing acute hydrops. According to a report by Ueji et al., the average age of corneal perforation in PMD is 50.1 ± 14.6 years, which is later than that in keratoconus (36.9 ± 16.3 years) 1). This reflects the slower progression of PMD compared to keratoconus. Perforation is a relatively rare complication, but once it occurs, it leads to severe visual impairment; therefore, monitoring progression, instructing patients to avoid eye rubbing, and controlling allergies are important. In PMD, because the thinning band is located in the peripheral region, local mechanical stress such as trauma, intraocular pressure fluctuations, or excessive eye rubbing can trigger perforation. Regular slit-lamp examination and corneal thickness measurement monitoring, as well as consideration of early surgical intervention in cases with significantly reduced corneal thickness, are recommended to prevent perforation.
Recent research topics related to PMD include the following:
Biomechanical early detection: Detection of PMD at the pre-onset stage (biomechanical stage) using corneal hysteresis, corneal resistance factor, and dynamic Scheimpflug analysis with devices such as the Ocular Response Analyzer and Corvis ST 2)
Personalized CXL: The sub400 protocol by Hafezi et al. adjusts irradiation time according to corneal thickness for ultrathin corneas less than 400 µm, demonstrating applicability to progressive cases previously contraindicated for conventional CXL9)
Simultaneous topography-guided PRK and CXL: A report by Stojanovic et al. achieved simultaneous improvement in visual function and inhibition of progression for PMD and keratoconus6)
Corneal allograft ICRS (CAIRS): Combined use of CAIRS using human corneal tissue and CXL has been reported, and a pilot study on keratoconus found no segment-related complications 11)
Genetic testing: Genetic testing that screens over 2,000 mutations in 75 genes including TGFBI is being put into practical use for risk assessment of corneal ectasia2)
AI analysis and epithelial thickness mapping: Efforts are underway to automatically detect pre-onset corneal ectasia using AI analysis of AS-OCT epithelial thickness maps and anterior segment images 2). Since the epithelium changes thickness to compensate for underlying stromal irregularity, epithelial thickness patterns are attracting attention as early markers of stromal ectasia
Ueji N, Kato K, Yonekawa Y, Takeuchi M, Takashima Y, Hirano K, et al. Case of unilateral pellucid marginal corneal degeneration progressing to corneal perforation with keratoconus in contralateral eye. American journal of ophthalmology case reports. 2022;25:101293. doi:10.1016/j.ajoc.2022.101293. PMID:35128154; PMCID:PMC8807968.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Belin MW, Asota IM, Ambrosio R Jr, Khachikian SS. What’s in a name: keratoconus, pellucid marginal degeneration, and related thinning disorders. Am J Ophthalmol. 2011;152(2):157-162.
Jinabhai A, Radhakrishnan H, O’Donnell C. Pellucid corneal marginal degeneration: A review. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2011;34(2):56-63. doi:10.1016/j.clae.2010.11.007. PMID:21185225.
Stojanovic A, Zhang J, Chen X, et al. Topography-guided transepithelial surface ablation followed by corneal collagen cross-linking performed in a single combined procedure for the treatment of keratoconus and pellucid marginal degeneration. J Refract Surg. 2010;26(2):145-152.
Raiskup-Wolf F, Hoyer A, Spoerl E, Pillunat LE. Collagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term results. Journal of cataract and refractive surgery. 2008;34(5):796-801. doi:10.1016/j.jcrs.2007.12.039. PMID:18471635.
Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK, United States Crosslinking Study Group. United States Multicenter Clinical Trial of Corneal Collagen Crosslinking for Keratoconus Treatment. Ophthalmology. 2017;124(9):1259-1270. doi:10.1016/j.ophtha.2017.03.052. PMID:28495149.
Hafezi F, Kling S, Gilardoni F, Hafezi N, Hillen M, Abrishamchi R, et al. Individualized Corneal Cross-linking With Riboflavin and UV-A in Ultrathin Corneas: The Sub400 Protocol. American journal of ophthalmology. 2021;224:133-142. doi:10.1016/j.ajo.2020.12.011. PMID:33340508.
Godefrooij DA, Gans R, Imhof SM, Wisse RP. Nationwide reduction in the number of corneal transplantations for keratoconus following the implementation of cross-linking. Acta ophthalmologica. 2016;94(7):675-678. doi:10.1111/aos.13095. PMID:27213687.
Jacob S, Patel SR, Agarwal A, Ramalingam A, Saijimol AI, Raj JM. Corneal Allogenic Intrastromal Ring Segments (CAIRS) Combined With Corneal Cross-linking for Keratoconus. Journal of refractive surgery (Thorofare, N.J. : 1995). 2018;34(5):296-303. doi:10.3928/1081597X-20180223-01. PMID:29738584.
Sykakis E, Karim R, Evans JR, Bunce C, Amissah-Arthur KN, Patwary S. Corneal collagen cross-linking for treating keratoconus. Cochrane Database Syst Rev. 2015;2015(3):CD010621. doi:10.1002/14651858.CD010621.pub2. PMID:25803325; PMCID:PMC10645161.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.