Salzmann nodular degeneration (SND) is a progressive, non-inflammatory corneal degenerative disease characterized by the formation of gray-white to blue-gray nodules in the subepithelial region on Bowman’s layer 1)9). It was first reported in 1925 by Austrian ophthalmologist Maximilian Salzmann and has since been classified as “Salzmann nodular degeneration” 1). The nodules are composed of hyaline-like material and fibrous tissue, and as they progress, they can extend to the central cornea, causing irregular astigmatism and visual impairment 1)10).
The prevalence is estimated at approximately 1 in 2,420 people, making it a rare disease 1). The age of onset is bimodal, with peaks in the 50s and 80s 1). In a retrospective study by Farjo et al. (93 cases), the mean age of onset was approximately 69 years for men and 52 years for women 6). The sex ratio shows a female predominance of 72–88%, and bilateral involvement is observed in 58–80% of cases, with nodules often forming in both eyes 1).
Nodules commonly occur in the mid-peripheral cornea and are often arranged in an arc along the limbus1). They can range from single to multiple, and in advanced cases, eight or more nodules may be present 1). In a comprehensive review by Maharana et al., it was noted that the frequency of SND increases with age, and a considerable number of cases are asymptomatic and overlooked 9). A management strategy review by Paranjpe et al., based on experience at Bascom Palmer Eye Institute, also characterizes SND as a rare disease, yet it is encountered with some frequency during preoperative screening for cataract surgery or corneal refractive surgery 7).
These chronic ocular surface inflammations and mechanical stimuli are thought to induce disruption of Bowman’s membrane and the epithelial basement membrane, triggering nodule formation 1).
QCan it occur in only one eye?
A
Bilateral cases account for 58–67% of reports, but unilateral cases are also seen in 30–40% of patients. When the underlying disease is bilateral, such as MGD or dry eye, bilateral involvement is common, while trauma or unilateral LASIK tends to result in unilateral disease.
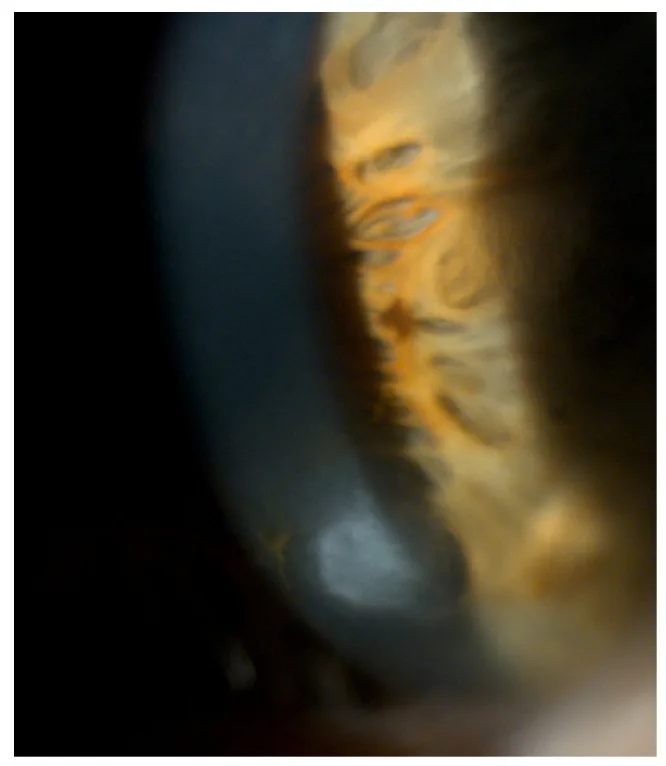
Roszkowska AM, Azzaro C, Calderone A, et al. Salzmann Nodular Degeneration in Ocular and Systemic Diseases. Journal of Clinical Medicine. 2024 Aug 20; 13(4900):$2. Figure 1. PMCID: PMC11355337. License: CC BY.
The slit lamp shows bluish-white nodules protruding forward from the corneal periphery. The three-dimensional appearance and superficial nature of Salzmann nodules are intuitively visible.
Asymptomatic: While nodules are confined to the periphery, subjective symptoms are often absent1). Not a few cases are discovered incidentally during health checkups or preoperative examinations for cataract surgery1)7).
Decreased visual acuity: When nodules reach the central cornea or cause irregular astigmatism due to surface irregularity, visual acuity decreases1). Ultra-high-resolution OCT can measure epithelial thinning and corneal surface elevation over nodules11).
Foreign body sensation: Due to nodular elevation and epithelial thinning over nodules, patients complain of foreign body sensation during blinking.
Glare and photophobia: Caused by light scattering due to irregular corneal surface1).
Epiphora and recurrent erosion: The epithelium over nodules becomes unstable, leading to recurrent corneal erosion and epiphora1).
Subepithelial nodules: Bluish-gray to gray-white elevated nodules are observed beneath the corneal epithelium1). They are usually 1–3 mm in diameter, single or multiple1)3).
Distribution of nodules: They preferentially occur in the mid-peripheral cornea, often arranged in an arc shape along the limbus1). In some cases, they show a flame-shaped distribution in the inferior quadrant1).
Epithelial thinning: The corneal epithelium over the nodules is thinned1)10).
Corneal surface irregularity: Surface elevation due to nodules and flattening between nodules can be detected by corneal topography1)7).
Secondary changes: Due to secondary degeneration, corneal opacity, conjunctival scarring, superficial corneal vessels, and limbal abnormalities from the underlying disease often coexist.
Limbal stem cell deficiency: In severe cases, limbal stem cell dysfunction accompanies, and nodules may form at the leading edge of conjunctival invasion. Extensive conjunctival invasion may require ocular surface reconstruction.
Histologically, disruption and loss of Bowman’s layer with deposition of hyaline-like material, fibrous tissue, and collagen proliferation are characteristic10). The nodules are paucicellular and composed of irregularly arranged collagen fibers and basement membrane-like material1)10).
Most SND develops as an acquired degeneration secondary to chronic ocular surface diseases or mechanical irritation. Major risk factors are listed below1)7)8).
Chronic blepharitis / Meibomian gland dysfunction (MGD): The most frequently associated ocular surface disease1)7). Tear film instability and chronic inflammation promote Bowman layer degeneration.
Dry eye: Increased tear evaporation and surface inflammation contribute1).
Long-term contact lens wear: Hamada et al. reported a high proportion of cases with a history of contact lens wear8). Chronic mechanical stimulation and hypoxia from long-term wear are involved.
Phlyctenular keratoconjunctivitis: A history of phlyctenules due to tuberculosis allergy or staphylococcal sensitization is a classic risk factor1).
Pterygium: Coexistence has been reported because it shares Bowman layer disruption and stromal fibroblast activation2).
After corneal refractive surgery: Onset after LASIK or PRK has been reported; in a review by Roszkowska, bilateral SND developed after LASIK in 5 young women aged 21–481). It tends to occur at the flap margin.
After cataract surgery: Cases have been reported where nodules formed at sites of incomplete healing of clear corneal incisions; the location of the clear corneal incision is closely related to the formation site of SND nodules1).
Corneal trauma: Cases after blunt trauma have been reported2).
In recent years, reports of association with systemic diseases have accumulated1). Most cases are bilateral; when bilateral SND of unknown cause is seen, it is recommended to search for underlying systemic disease.
Connective tissue diseases / Skin diseases
Ehlers-Danlos syndrome: Shares connective tissue fragility; reported as a case of recurrent bilateral SND after LASIK1).
Dermatopathia pigmentosa reticularis: An autosomal dominant skin pigmentary disorder associated with extensive corneal nodules1).
Inflammatory / Syndromic / Endocrine diseases
Crohn disease: Chronic gastrointestinal inflammation; there are case reports of SND recurrence linked to disease activity1).
Kabuki syndrome: A multiple malformation syndrome with reported bilateral midperipheral SND1).
Kartagener syndrome: Associated with ciliary dyskinesia; case reports of flame-shaped SND in the inferior cornea1).
Thyroid eye disease: An association via chronic ocular surface inflammation has been suggested1).
Some familial cases show an autosomal dominant inheritance pattern, and mutations in the TGFBI gene, known to cause corneal dystrophies, have been detected in some SND patients1). However, most SND is acquired secondary degeneration, and heredity is not the main cause.
QIs contact lens wearing related?
A
Long-term contact lens wear causes chronic mechanical irritation and tear film instability, and has been repeatedly reported as a risk factor for SND. Wearers, especially those who wear lenses for long hours, are recommended to have regular eye exams to evaluate the corneal surface.
The diagnosis of SND is primarily clinical based on slit-lamp microscopy findings. Imaging is useful for assessing the extent and depth of lesions and for evaluating the impact on surgical planning such as cataract surgery1)7).
Examination Method
Main Findings
Significance
Slit-lamp microscopy
Subepithelial blue-gray nodules, midperipheral distribution
Irregular fibrillar structures, loss of keratocytes
Pathological evaluation1)12)
Slit-lamp examination: Direct observation of bluish-gray to gray-white elevated nodules. Assess the number, size, distribution, and involvement of the central cornea, along with the presence of blepharitis or MGD in the background1)2).
Corneal topography (Placido-based): Quantitative evaluation of surface irregularity and irregular astigmatism caused by nodules1). Nodules show characteristic flattening over the nodule and steepening between nodules. Corneal shape changes affect IOL power calculation for cataract surgery, making preoperative assessment important1).
Anterior segment OCT (AS-OCT): Non-invasively visualizes nodules as hyperreflective subepithelial deposits and assesses their relationship with Bowman’s layer and depth1)11). Ultra-high-resolution OCT can measure internal structure and thickness of nodules in detail11). Preoperative AS-OCT assessment of nodule and opacity depth helps determine whether superficial keratectomy, PTK, or deeper surgery is needed.
In vivo confocal microscopy (IVCM): Allows cellular-level observation of nodule microstructure, characteristically showing irregular fibrous structures, loss of keratocytes, and decreased subepithelial nerve plexus density1)12). Epithelial cells over nodules exhibit CK19-positive transit amplifying cell properties, suggesting epithelial differentiation abnormalities1)12).
It is important to differentiate from diseases presenting with subepithelial nodules1)2).
Band keratopathy: A gray-white band-shaped opacity caused by calcium deposition in Bowman’s membrane. It extends horizontally from the 3 and 9 o’clock positions, leaving a clear zone (limbal clear zone) between the limbus and the lesion. It differs significantly from SND in that it responds to EDTA chelation.
Climatic droplet keratopathy / spheroidal degeneration: Multiple yellow to amber granular deposits occur in the exposed area of the cornea. It is known to be associated with exposure to ultraviolet light and dry environments.
Herpetic stromal keratitis: May present with nodular inflammatory lesions, but is differentiated by decreased corneal sensation, opacity, inflammatory findings, and acute course of vision loss 2).
Phlyctenular keratoconjunctivitis: Forms round small nodules with blood vessels at the limbus or peripheral cornea, and develops as a delayed-type hypersensitivity reaction to tuberculosis or Staphylococcus aureus 2).
Ocular surface squamous neoplasia (OSSN): An epithelial mass arising near the limbus, characterized by neovascularization and gelatinous elevation. Cytology or biopsy is useful for differentiation.
Marginal corneal ulcer / catarrhal ulcer: Peripheral corneal infiltration and ulcer associated with blepharitis, differentiated by the course of the lesion and inflammatory findings.
Pericentral hypertrophic subepithelial corneal degeneration (PHSCD): A rare degeneration presenting with subepithelial opacity in the paracentral area, differing in that the opacity spreads in a band-like pattern rather than nodular form.
In a case series by Kuan et al., three cases presenting with corneal nodules were reported, with final diagnoses of herpetic stromal keratitis, phlyctenular keratoconjunctivitis, and SND, respectively 2). Differentiation of corneal nodules is performed by combining detailed history taking (previous eye diseases, trauma, contact lens use, refractive surgery history), slit-lamp findings (location, color, presence of blood vessels, corneal sensation), and depth assessment using AS-OCT2). The time course of onset is also important; SND progresses gradually over months to years, whereas infectious or inflammatory nodules develop and progress over a relatively short period 2).
Treatment is selected stepwise according to the location, size, severity of symptoms, and impact on visual function 1)4)7). Asymptomatic or peripherally localized SND often requires only observation 1).
For asymptomatic or mild cases, conservative treatment is the mainstay. Since control of the underlying chronic ocular surface disease is directly linked to prevention of recurrence, management of the primary disease is the highest priority 1)7).
Artificial tears / hyaluronic acid eye drops: Used frequently to stabilize the tear film and protect the corneal epithelium. Preservative-free formulations are preferable.
Surgical treatment is selected based on the depth of the nodules. The AAO Corneal Edema and Opacification Preferred Practice Pattern also recommends three stages for managing subepithelial fibrosis such as SND: epithelial debridement (ED), superficial keratectomy (SK), and PTK4).
Nodule Excision / Superficial Keratectomy
Method: Grasp the nodule with forceps and bluntly dissect and remove it at the Bowman’s membrane level 1)4). Sometimes the abnormal epithelium and nodule are removed together using a corneal blade such as a golf knife.
Success rate: Superficial keratectomy alone achieves visual improvement in approximately 90% of cases 1). Postoperatively, corneal flattening may alter astigmatism and refractive power.
Method: Excimer laser is used to uniformly ablate superficial tissue including nodules 1)4). This is chosen for cases with deep opacity or when superficial keratectomy does not provide adequate smoothing.
Advantages: A uniform and smooth corneal surface is obtained, improving postoperative optical quality4).
MMC combination: The use of mitomycin C (MMC) can suppress postoperative corneal haze1)4).
Preoperative evaluation: Anterior segment OCT is used to assess the thickness of nodules and deep opacities, and to determine the depth of excision11).
For nodule excision and PTK, PTK smoothing is considered particularly effective in cases where opacities remain under Bowman’s layer. Understanding the depth of involvement via anterior segment OCT is important for selecting the surgical technique.
In severe cases, i.e., those with extensive nodular distribution and conjunctival invasion accompanied by limbal stem cell deficiency, removal of abnormal conjunctival epithelium and ocular surface reconstruction are necessary. Limbal transplantation or corneal epithelialization is selected, and long-term maintenance therapy including topical steroids to suppress rejection, therapeutic contact lens wear, anti-inflammatory treatment, immunosuppression, and superficial epithelial protection is required postoperatively. Furthermore, in cases where opacities extend into the deep stroma, lamellar keratoplasty (DALK) or penetrating keratoplasty (PKP) may be necessary, though this is not frequent1).
Recurrence after surgical treatment is an important issue in SND management. In a retrospective study of 93 cases by Farjo et al., recurrence was observed in approximately 22% over a mean follow-up of 61 months6). Yoon and Park from Korea also reported cases of bilateral recurrent SND in Jpn J Ophthalmol, indicating a tendency for higher recurrence in bilateral cases and those with systemic comorbidities5).
The key to preventing recurrence is continuous management of the underlying chronic ocular surface disease1)5)7). Controlling blepharitis, MGD, and dry eye, quelling inflammatory diseases, correcting contact lens wear, and managing systemic disease activity are thought to reduce postoperative recurrence rates. In their management strategy review, Paranjpe et al. state that nodules located deeper are more difficult to remove and have a higher recurrence risk, and in such cases, a multi-step approach combining superficial keratectomy with PTK to ensure corneal surface smoothing and MMC to suppress haze and fibrotic recurrence is useful7). In their review, Maharana et al. also emphasize that continuing conservative therapy (artificial tears, steroids, eyelid hygiene) postoperatively is essential for suppressing recurrence9).
For patients with SND, lifestyle guidance should be provided based on the understanding that the epithelium around the nodules is unstable. It is advisable to avoid vigorous eye rubbing, prolonged contact lens wear, and exposure to dust or dry environments. Even if symptoms are mild, anti-inflammatory eye drops and artificial tears should be continued, and regular slit-lamp microscopy and corneal topography should be performed to monitor the condition. When cataract surgery is planned, since the nodules affect surgical planning, it is recommended to first treat the SND to stabilize the corneal shape before calculating the IOL power1)7).
QDoes it recur after surgery?
A
Recurrence after surgical treatment is an important issue, with recurrence reported in approximately 22% of cases over an average follow-up of about 5 years. Recurrence tends to be more common in bilateral cases and those with underlying systemic diseases. Persistent management of background ocular surface diseases such as blepharitis, MGD, and dry eye is most important for preventing recurrence.
6. Pathophysiology and Detailed Mechanism of Onset
The pathology of SND is understood as a series of fibrotic processes beginning with disruption of Bowman’s layer and the epithelial basement membrane1)10).
Disruption of Bowman’s layer: Chronic inflammation, mechanical stimulation, or trauma cause micro-tears in Bowman’s layer and the epithelial basement membrane1)10).
Migration of corneal stromal cells: Corneal keratocytes migrate through the disrupted areas into the subepithelial region1).
Differentiation into myofibroblasts: The migrated corneal cells differentiate into myofibroblasts1)10).
Deposition of fibrous extracellular matrix: Myofibroblasts produce and deposit fibrous ECM mainly composed of hyalinized collagen, forming nodules1)10).
This process repeats as long as the underlying chronic ocular surface inflammation or mechanical stimulation persists, leading to an increase in the number and size of nodules.
Nodule formation in SND is thought to involve three factors: matrix metalloproteinase-2 (MMP-2), platelet-derived growth factor (PDGF), and transforming growth factor β1 (TGF-β1)1).
MMP-2: Degrades type IV collagen, a major component of the epithelial basement membrane, facilitating the migration of PDGF and TGF-β1 into the stroma 1).
PDGF: Promotes migration and proliferation of corneal stromal cells 1).
TGF-β1: Induces differentiation of corneal stromal cells into myofibroblasts and enhances production of fibrous ECM 1).
Epithelium-derived enzymes: The nodular epithelium shows high proliferative activity and expresses enzymes such as α-enolase at high levels 1).
In the corneal epithelium overlying the nodule, CK19-positive transit amplifying cells are observed, while expression of CK3/12 (markers of fully differentiated epithelial cells) and the stem cell marker ABCG2 is reduced 1)12). That is, the epithelium over the nodule is in an intermediate state between stem cells and fully differentiated cells, suggesting that abnormal epithelial differentiation may be involved in nodule formation 1)12).
Histologically, the interior of the nodule is poor in cellular components and consists of irregularly arranged collagen fibers, hyaline-like material, and basement membrane-like material 10). Part of Bowman’s layer is absent, and fibrous tissue deposited on it lifts the epithelium, appearing as a raised nodule.
When chronic blepharitis, MGD, or dry eye is present as a background of SND, instability of the tear film and persistent inflammatory cytokines form a vicious cycle that promotes nodule formation. Disruption of Bowman’s layer and activation of myofibroblasts can recur repeatedly unless the underlying disease is resolved. Therefore, even if the nodule is removed alone, recurrence is likely if the primary disease remains. As a treatment strategy, it is essential to combine conservative therapy to control the underlying disease and surgical removal of the nodule 1)7)9).
Hypothesis of epithelial differentiation abnormality
The finding that epithelial cells over the nodule are in an intermediate differentiation state supports the view that SND is not merely stromal fibrosis but a result of disrupted homeostasis among the epithelium, Bowman’s layer, and stroma 1)12). In the normal cornea, cells derived from epithelial stem cells at the limbus differentiate and migrate regularly toward the center, but over SND nodules, this differentiation process is thought to be partially arrested, leading to local accumulation of transit amplifying cells. This epithelial change may provide a basis for promoting disruption of the underlying Bowman’s layer and stromal fibrosis.
In some familial SND cases, an autosomal dominant inheritance pattern has been reported, and mutations in the TGFBI gene, known to cause corneal dystrophy, have been detected in some SND patients 1). With advances in genomic analysis, the relationship between genetic predisposition and the pathogenesis of SND is expected to become clearer.
In recent years, associations with various systemic diseases such as Ehlers-Danlos syndrome, Crohn’s disease, Kabuki syndrome, Kartagener syndrome, dermatopathia pigmentosa reticularis, and thyroid eye disease have been reported 1). These associations may be based on common inflammatory pathways or connective tissue fragility, providing a perspective to reconsider SND not as a “localized corneal degeneration” but as a “manifestation of systemic inflammatory conditions on the ocular surface.”
Case reports of concurrent keratoconus and SND are accumulating 3). Both keratoconus and SND share Bowman’s layer disruption and activation of corneal stromal cells, and it has been suggested that they may have common risk factors such as ocular surface inflammation and mechanical stimulation (eye rubbing, contact lens wear) 3). When bilateral SND is observed in young patients, active evaluation for concurrent keratoconus using Pentacam or anterior segment OCT is recommended.
Quantitative assessment of nodule depth and internal structure using ultra-high-resolution anterior segment OCT and spectral-domain OCT is advancing 11), improving the precision of surgical technique selection. By objectively measuring nodule thickness, boundaries, and the condition of the underlying stroma, criteria are being developed to determine whether superficial keratectomy alone is sufficient, whether PTK is needed, or whether MMC should be combined. Additionally, quantitative evaluation of epithelial differentiation abnormalities and nerve plexus changes using IVCM may be applied to early detection of pathology and assessment of treatment efficacy 12). In the future, combining these with measurement of systemic diseases and inflammatory biomarkers is expected to lead to risk stratification and personalized treatment for SND.
QAre there genetic factors?
A
In some families, an autosomal dominant inheritance pattern has been reported, and mutations in the TGFBI gene have been detected in some SND patients. However, most SND cases are acquired degeneration secondary to chronic ocular surface disease, and genetic causes are rare. Genetic testing is considered only in cases of early onset or strong family history.
Roszkowska AM, Azzaro C, Calderone A, Spinella R, Schiano-Lomoriello D, Mencucci R, Wylegala A. Salzmann Nodular Degeneration in Ocular and Systemic Diseases. J Clin Med. 2024;13(16):4900. doi:10.3390/jcm13164900
Kuan HC, Cheng EYI, Yong MH, Wan Abdul Halim WH, Othman O. Corneal Nodules and Possible Pathologies: A Case Series. Cureus. 2021;13(12):e20822. doi:10.7759/cureus.20822
Das D, Lomi N, Sasi A, Kumari N, Muraleekrishna M, Tandon R. Layers of Rarity: An Unusual Concurrence of Keratoconus, Salzmann’s Nodular Degeneration, Ptosis, and Congenital Retinal Macrovessel. Cureus. 2025;17(9):e92115. doi:10.7759/cureus.92115
American Academy of Ophthalmology Cornea/External Disease Panel. Corneal Edema and Opacification Preferred Practice Pattern. Ophthalmology. 2024.
Hamada S, Darrad K, McDonnell PJ. Salzmann’s nodular corneal degeneration (SNCD): Clinical findings, risk factors, prognosis and the role of previous contact lens wear. Cont Lens Anterior Eye. 2011;34(4):173-178. doi:10.1016/j.clae.2011.02.004
Maharana PK, Sharma N, Das S, Agarwal T, Sen S, Prakash G, Vajpayee RB. Salzmann’s Nodular Degeneration. Ocul Surf. 2016;14(1):20-30. doi:10.1016/j.jtos.2015.08.006
Stone DU, Astley RA, Shaver RP, Chodosh J. Histopathology of Salzmann nodular corneal degeneration. Cornea. 2008;27(2):148-151. doi:10.1097/ICO.0b013e31815a50fb
Hurmeric V, Yoo SH, Karp CL, Galor A, Vajzovic L, Wang J, Dubovy SR, Forster RK. In vivo morphologic characteristics of Salzmann nodular degeneration with ultra-high-resolution optical coherence tomography. Am J Ophthalmol. 2011;151(2):248-256.e2. doi:10.1016/j.ajo.2010.08.013
Roszkowska AM, Spinella R, Aragona P. Morphologic and confocal investigation on Salzmann nodular degeneration of the cornea. Invest Ophthalmol Vis Sci. 2011;52(8):5910-5919. doi:10.1167/iovs.11-7789.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.