Calcific band keratopathy (CBK) is a chronic corneal degeneration characterized by the deposition of inorganic phosphates and carbonates, mainly calcium hydroxyapatite, in the subepithelium, Bowman’s layer, and anterior stroma 1). The first description of this condition is attributed to Dixon in 1948, and it has since been widely recognized as a secondary degeneration associated with chronic ocular diseases and systemic metabolic disorders 1, 7). The deposits are primarily calcium crystals, but may be mixed with non-crystalline phosphates, carbonates, or elastoid-degenerated collagen, in which case the response to chelating agents is poor 1).
This condition is characterized by band-shaped gray-white opacities in the horizontal interpalpebral zone, leaving a clear zone between the opacity and the limbus. Progression is generally slow; while the opacity remains in the peripheral cornea, it is asymptomatic, but when it reaches the pupillary area, it causes visual impairment, photophobia, and pain or foreign body sensation due to epithelial erosion 4). If the underlying disease is not well controlled, recurrence after treatment is possible 8).
In adults, it often occurs secondary to long-standing chronic uveitis, silicone oil-filled eyes, or refractory glaucoma. In children, it is frequently seen as a late complication of chronic iridocyclitis associated with juvenile idiopathic arthritis (JIA), and is often discovered together with complicated cataract and posterior synechiae during the course of “white uveitis” with few subjective symptoms 6). Systemic backgrounds include metabolic and inflammatory diseases such as hyperparathyroidism, chronic renal failure, and sarcoidosis. Given this diversity, calcific band keratopathy should be understood not as a single disease but as a “syndrome with calcium deposition as its clinical feature” 7).
The typical age of onset depends on the underlying disease: in JIA-associated chronic iridocyclitis, it often occurs from school age to adolescence; in cases with silicone oil retention, it occurs from several months to several years after surgery; and in hypercalcemia cases, it often occurs after middle age. It can be either bilateral or unilateral, but when associated with systemic disease, it tends to be bilateral 10).
QWhat is the recurrence rate of band keratopathy?
A
The recurrence rate after EDTA chelation therapy is reported to be approximately 17.8% 1). Recurrence is higher in cases with persistent underlying diseases such as uveitis or corneal herpes1, 8). The combination of topography-guided PRK and therapeutic laser keratectomy may contribute to reducing recurrence rates by improving surface smoothness and tear film stability 1).
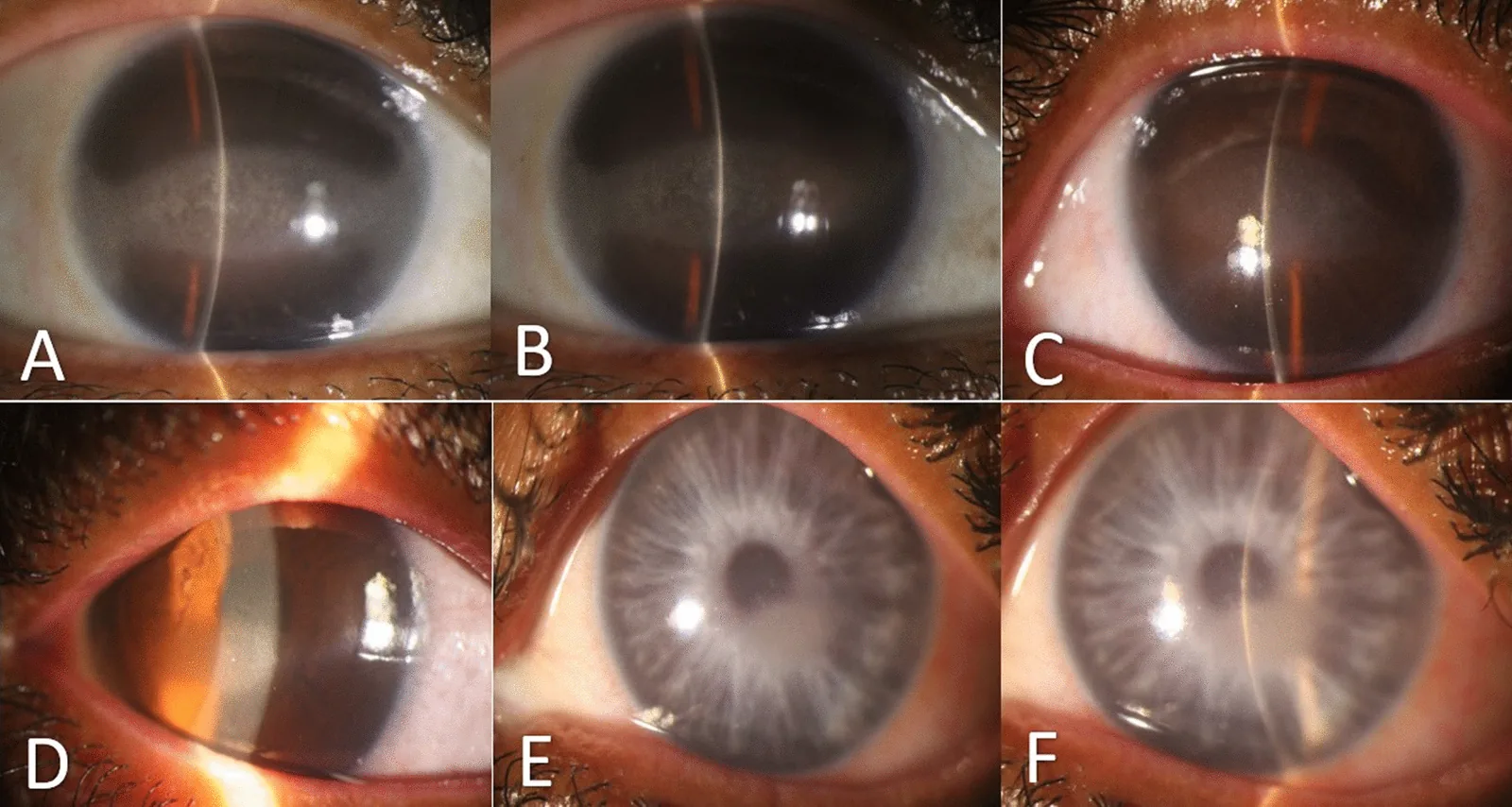
Abdi P, et al. Familial primary calcific band-shaped keratopathy with late onset systemic disease: a case series and review of the literature. J Med Case Rep. 2024. Figure 1. PMCID: PMC10925011. License: CC BY.
Preoperative slit-lamp photographs of three Iranian siblings (A, B: right and left eyes of a 41-year-old sister; C, D: right and left eyes of a 37-year-old brother; E, F: right and left eyes of a 33-year-old sister). These correspond to “band keratopathy” discussed in the section “2. Main Symptoms and Clinical Findings.”
Mild cases are often asymptomatic. When the lesion covers the pupillary area, visual impairment, photophobia, and foreign body sensation appear 4). Light scattering by calcium crystals causes glare and reduced contrast sensitivity1). In advanced cases with epithelial erosion or epithelial defects, severe pain and tearing may occur. Awareness of visual loss often becomes clear only when deposits reach the central pupillary area; glare, blurred vision, and decreased night vision may be preceding symptoms. In unilateral cases, it may be noticed by comparison with the other eye. Cases with recurrent corneal erosions are characterized by severe pain and tearing upon waking.
Opacification begins in the peripheral cornea of the interpalpebral fissure horizontally (at 3 and 9 o’clock). A 1-2 mm wide clear zone (limbal clear zone) exists between the limbus and the deposits, which is a morphological feature of this disease. The opacification gradually progresses toward the center and fuses into a band shape. Within the opacity, there are scattered Swiss cheese-like clear holes, corresponding to the penetration points of corneal nerves through Bowman’s layer. Advanced cases may involve epithelial irregularity, recurrent epithelial defects, and anterior stromal opacity 7).
On imaging, confocal microscopy shows deposits as highly reflective, thick cumulus-like structures, and acoustic shadowing within the deposits is also observed. Anterior segment optical coherence tomography (AS-OCT) can quantitatively assess the depth and thickness of the deposit layer as a hyperreflective signal; a case report confirmed a deposit layer extending to approximately 150 μm 1). Corneal topography can quantify irregularity using the corneal morphology index (CMI) 1).
The distribution pattern of deposits provides clues for estimating the pathology. In cases associated with chronic uveitis, a typical pattern of centripetal progression from the 3 and 9 o’clock positions of the interpalpebral fissure is often observed, while in JIA-related cases, severe cases that progress to the central area with obscuration of the clear zone are also experienced 6). In cases of occupational mercury vapor exposure, irregular deposits may occur near the central cornea, and history taking is key to differential diagnosis 1). In advanced cases, tear film breakup time shortening and epithelial microdefects due to corneal surface irregularity are observed, and fluorescein staining under slit lamp shows a punctate keratopathy-like staining pattern. In cases with a history of recurrent corneal epithelial erosion, it is presumed that Bowman’s layer disruption is the underlying cause 7).
Band keratopathy is secondary to various ocular and systemic diseases. Clinically common causes include chronic intraocular inflammatory diseases, hypercalcemia, and silicone oil injection after vitrectomy. Causes may exist alone or overlap; for example, in long-term uveitis cases, inflammation, phosphate-containing steroid eye drops for secondary glaucoma, and hypercalcemia may all be involved simultaneously.
Ocular Causes
Chronic uveitis: One of the most common ocular causes, where persistent intraocular inflammation promotes calcium deposition 2, 7)
Juvenile idiopathic arthritis-associated chronic iridocyclitis: Band keratopathy is frequently observed along with complicated cataract and posterior synechiae, and is a major late complication 6)
Secondary glaucoma: May occur in long-standing glaucoma cases, especially those with decreased corneal endothelial function 2)
Corneal stromal keratitis: Chronic herpetic stromal keratitis or interstitial keratitis as the underlying condition
After silicone oil injection: Long-term retention after vitrectomy induces corneal degeneration
Corneal exposure: Persistent dryness due to lagophthalmos or facial nerve palsy is involved
Systemic Causes
Primary hyperparathyroidism: A representative systemic cause mediated by hypercalcemia
Chronic renal failure/dialysis patients: Metastatic calcification due to elevated serum calcium-phosphate product causes calcification of the conjunctiva and cornea5, 10)
Sarcoidosis, vitamin D intoxication: Hypercalcemia due to granulomatous diseases as the background
Occupational exposure: Cases of exposure to mercury vapor or calcium chromate vapor have been reported 1)
Phosphate-containing steroid eye drops: Long-term use may lead to deposition in the cornea as precipitates.
The exact mechanism of calcium deposition is not fully understood, but increased tissue pH and enhanced tear evaporation are thought to be major factors. In the interpalpebral fissure, tears are exposed to the atmosphere and carbon dioxide is released, raising tear pH and reducing the solubility of calcium salts. Tear evaporation is greater in areas with a wider palpebral fissure, and the fact that the interpalpebral fissure dries more easily at room temperature than the lid margin supports the distribution of deposits coinciding with the palpebral fissure. Dry eye is an exacerbating factor through increased tear evaporation and tissue hyperosmolarity, and chronic instability of the ocular surface contributes to the progression of this condition 5). In chronic renal failure cases, in addition to an elevated serum calcium-phosphate product, a mechanism of metastatic calcification is postulated, where calcium salts carried by blood flow from limbal vessels deposit under the epithelium 5, 10).
Risk factors are summarized in the table. In cases with multiple coexisting factors, the latency period before onset tends to be shorter. In chronic iridocyclitis associated with juvenile idiopathic arthritis, band keratopathy may become apparent several years after diagnosis, and regular anterior segment screening is important 6). In pediatric cases, subjective symptoms are often not reported, so it is desirable to detect the condition early through regular examinations before visual loss or foreign body sensation occurs.
The triad of band-shaped gray-white opacity, Swiss cheese-like appearance, and clear zone between the opacity and the limbus is characteristic clinical findings, and diagnosis is possible by slit-lamp microscopy 4). With slit-lamp retroillumination, the deposits appear as shadows, making it easy to visually assess the extent and density of deposits. AS-OCT is useful for evaluating the depth and thickness of deposits and extension into the anterior stroma, and serves as an indicator for treatment selection 1). Corneal topography is used for quantitative assessment of corneal irregularity, and can objectively track changes in CMI before and after treatment 1). Confocal microscopy allows observation of deposits as highly reflective structures and also evaluates the degree of damage to the subbasal nerve plexus, which is helpful for understanding the pathology in cases with recurrent epithelial erosion. Ultrasound biomicroscopy (UBM) is a useful ancillary examination for evaluating structures from the anterior cornea to the limbus.
Vogt’s limbal girdle is an age-related fine calcium salt deposition in the peripheral cornea, often seen in healthy individuals as an asymptomatic aging change4). It occurs adjacent to the limbus and does not progress toward the center of the palpebral fissure, distinguishing it from band keratopathy. Spheroidal degeneration (climatic droplet keratopathy) is a subepithelial deposition of hyaline-like material; its morphology is similar to band keratopathy but the deposits differ in nature, commonly seen in outdoor workers in areas with strong UV exposure, characterized by golden to yellowish-brown oil droplet-like globules. Secondary corneal amyloidosis also produces white deposits in the palpebral fissure area and requires differentiation, diagnosed by Congo red positivity and birefringence under polarized light. Gelatinous drop-like corneal dystrophy is a juvenile-onset epithelial amyloidosis that presents with mulberry-like or band-shaped opacities, and its appearance is similar, so caution is needed.
QWhat tests are necessary to confirm band keratopathy?
A
In many cases, diagnosis is possible based solely on typical clinical findings with a slit-lamp microscope. AS-OCT is useful for quantitative assessment of the depth of deposits and helps in selecting treatment 1). With a confocal microscope, deposits appear highly reflective. Blood tests such as serum calcium, phosphate, renal function, and ACE levels are performed to search for underlying causes. In bilateral pediatric cases, evaluation of anterior chamber inflammation is also important, keeping in mind juvenile idiopathic arthritis-associated chronic iridocyclitis 6).
If there is no visual impairment or symptoms, observation is generally the principle 4). Active treatment is initiated when symptoms appear. Treatment methods are broadly classified into three types: local removal with a needle, chelation with drug application, and excimer laser corneal ablation.
When calcium deposits are locally protruding or plate-like, there is a simple method of flipping the deposits off using a 27-gauge needle. However, the stroma directly beneath the deposits is often thin, and cutting into the deep stroma can cause iatrogenic scarring, so caution is required.
This is the most widely used treatment 4, 7, 8). After mechanical removal of the corneal epithelium, a cotton swab soaked in ethylenediaminetetraacetic acid (EDTA) solution is applied to the calcium deposits, and the deposits are scraped off with a golf knife or similar instrument. The standard concentration is 0.4–1% EDTA solution or 0.05 mol/L EDTA-Na, and finally, the area is washed with a sufficient amount of phosphate buffer or saline. A long-term follow-up study reported in 2004 showed that while EDTA chelation achieves mean visual improvement, recurrence is high in cases with persistent underlying disease 8). For band keratopathy as a complication of juvenile idiopathic arthritis-associated chronic iridocyclitis, treatment with EDTA or dilute hydrochloric acid, as well as excimer laser, is performed 6).
Conventional Na2EDTA became difficult to obtain and expensive after the US FDA withdrew approval, and an alternative preparation method using K2EDTA blood collection tubes has been proposed 3). The simple method of preparing from the inner wall of K2EDTA-coated blood collection tubes has been confirmed safe and effective in multiple reports 2, 3).
K2EDTA (derived from blood collection tubes)
Features: A simple method of dissolving and preparing from the K2EDTA coating on the inner wall of lavender-cap blood collection tubes 3)
Advantages: Inexpensive ($36–47 per 100 tubes, lower cost compared to Na2EDTA average $117) and readily available 3)
Efficacy: Calcium removal effect equivalent to Na2EDTA has been confirmed in multiple clinical cases 2, 3)
Safety: No adverse effects on corneal endothelium or delayed healing have been reported. Concurrent performance with cataract surgery or corneal endothelial transplantation is also safe2)
Indications: Cases unresponsive to EDTA, deep deposits, mixed non-calcified deposits, and cases with irregular astigmatism1, 9)
Standard technique: Irradiation is performed with the epithelium left intact, at a diameter of approximately 7 mm and a depth of approximately 100 μm. A 1% hydroxymethylcellulose solution is used as a masking agent1)
Combined topography-guided PRK: To correct irregular astigmatism and optimize visual quality, aberrations of the anterior and posterior segments are comprehensively corrected1)
Precautions: Postoperative hyperopia of approximately 3 D and sufficient corneal thickness (preoperative thickness of at least 450 μm as a guideline) are required9)
K2EDTA Preparation Method
Concentration
Preparation Time
Method 1 (5-vial transfer method)
65 mg/mL3)
189 seconds3)
Method 2 (1-vial shaking method)
35 mg/mL3)
38 seconds3)
Method 3 (cotton swab dissolution method)
52 mg/mL3)
83 seconds3)
The standard preparation concentration of Na2EDTA is 30–40 mg/mL, and Method 3 can achieve a higher concentration in a short time, making it recommended as the best balance of concentration, preparation time, and simplicity3).
Therapeutic Laser Corneal Ablation (PTK) Combined with PRK
Therapeutic laser corneal ablation (phototherapeutic keratectomy: PTK) using excimer laser has been established as an effective treatment for removing deep deposits and mixed-type material since the long-term follow-up study by O’Brart et al. in 19939). In recent years, individualized surgery combining topography-guided transepithelial PRK and PTK has made it possible to simultaneously achieve deposit removal and irregular astigmatism correction1). In a case of band keratopathy due to mercury vapor exposure (63-year-old male), after EDTA was ineffective, topography-guided PRK+PTK was performed, improving right eye uncorrected visual acuity (UCVA) from 20/100 to 20/20 and left eye from 20/200 to 20/631). The corneal morphology irregularity index (CMI) also significantly improved from 15 to 3 μm in the right eye and from 21 to 11 μm in the left eye1).
Postoperative management is common to both EDTA chelation and PTK/PRK: a therapeutic soft contact lens is placed, and antibiotic eye drops and low-dose steroid eye drops are administered to promote rapid epithelial regeneration. Early postoperative pain management and infection prevention are important. Epithelialization usually takes 5–7 days, and during that period, follow-up evaluates the area of epithelial defect, presence of anterior chamber inflammation, and contact lens fitting status. In cases with underlying chronic uveitis, adequate anti-inflammatory treatment should be achieved preoperatively, and anti-inflammatory therapy should be continued postoperatively to reduce the risk of recurrence6, 8).
Visual prognosis depends on control of the underlying disease and the depth of deposits. For superficial deposits alone, EDTA chelation alone can achieve good visual improvement, but for deep deposits extending to the anterior stroma, PTK is required, and irregular astigmatism may persist postoperatively1, 9). In cases with severe corneal scarring or combined endothelial dysfunction, lamellar keratoplasty (DALK) or penetrating keratoplasty (PKP) may ultimately be chosen7).
QIs it safe to prepare K2EDTA from blood collection tubes?
A
The method of extracting K2EDTA from blood collection tubes for the treatment of band keratopathy has been confirmed safe and effective in multiple reports 2, 3). No adverse effects on the corneal endothelium or delayed healing have been reported 3). Simultaneous surgery with cataract surgery or corneal endothelial transplantation can also be performed safely 2).
The essence of this disease is the deposition of calcium hydroxyapatite in the corneal epithelial basement membrane, Bowman’s layer, and anterior stroma 1, 4). Deposits may include mixed substances such as amorphous phosphates, carbonates, and elastoid-degenerated collagen, and the presence of mixed substances may cause poor response to EDTA chelation therapy 1, 7).
The reason for the band-shaped distribution along the interpalpebral fissure is thought to be mainly due to increased tear pH and enhanced evaporation. In the interpalpebral zone, tears are exposed to air and carbon dioxide is released, causing a local pH increase, which reduces the solubility of calcium salts (especially calcium phosphate and calcium carbonate), promoting deposition. Ocular surface stress such as increased tear evaporation, dry eye, and hyperosmolarity also promote deposition 5).
When calcium deposition is severe, Bowman’s layer is damaged and disrupted, leading to abnormal adhesion of the overlying corneal epithelium. This mechanism causes recurrent epithelial erosions and chronic pain 7). In chronic uveitis, inflammatory cytokines and increased calcium ions in the aqueous humor penetrate from the posterior cornea, promoting deposition through chronic corneal endothelial and stromal stress 6).
Band keratopathy in chronic renal failure involves both metastatic calcification and chronic systemic inflammation 5, 10). When the serum calcium-phosphorus product is high, calcium salts are more likely to deposit in the subepithelial tissue via blood flow from limbal vessels. In dialysis patients, hyperparathyroidism (secondary or tertiary) often coexists, and calcium metabolism abnormalities underlie the corneal pathology 10). Persistent serum calcium-phosphorus product exceeding 70 mg²/dL² is known to clearly increase the risk of corneal and conjunctival calcification, and correction of mineral metabolism in dialysis management is the basis for preventing this disease 10).
At the molecular level, it has been suggested that local increases in inflammatory cytokines and alkaline phosphatase activity may promote nucleation of calcification. The aqueous humor in chronic uveitis contains high concentrations of inflammatory cytokines, which are thought to contribute to deposit formation via diffusion from the posterior corneal surface into the stroma 6, 7). Increased tear osmolarity due to dry eye, chronic mechanical stimulation of the palpebral fissure area, and long-term exposure to eye drops containing phosphate buffer (such as some steroid eye drops) have also been reported as risk factors, and consideration of formulation selection is necessary to reduce iatrogenic onset 5).
QHow deep into the cornea do the deposits of band keratopathy extend?
A
Typically, they remain in the subepithelial layer to Bowman’s layer. However, in advanced cases, they can extend to the anterior stroma, and a report has confirmed deposits of approximately 150 μm on AS-OCT1). In cases with deep deposits, EDTA chelation alone is insufficient, and laser treatments such as therapeutic laser keratectomy are required 1, 9).
The combination of topography-guided transepithelial PRK and therapeutic laser keratectomy has been reported as a powerful treatment option for EDTA-resistant cases 1). Ray-tracing algorithms allow integrated correction of anterior and posterior segment aberrations, minimizing stromal consumption while optimizing visual quality. Corneal transparency and visual improvement were maintained at 6 months postoperatively 1).
Simplification of preparation methods using K2EDTA blood collection tubes is also progressing, enabling lower-cost and faster treatment compared to conventional Na2EDTA 2, 3). Recently, reports of simultaneous performance with cataract surgery through clear corneal incisions and corneal endothelial transplantation have expanded the flexibility of vision recovery strategies 2).
Future challenges include optimizing personalized treatment combining EDTA, PTK, amniotic membrane transplantation, and topography-guided PRK, as well as establishing recurrence prevention strategies linked to treatment of underlying diseases (molecular targeted therapy for chronic uveitis, surgical treatment for hyperparathyroidism, phosphate metabolism management in dialysis patients) 6, 8).
With the introduction of biologics (adalimumab, infliximab, etc.) for juvenile idiopathic arthritis-associated uveitis, control of intraocular inflammation has become more stable than before, which may lead to suppression of new onset and recurrence of band keratopathy in the long term 6). Indeed, cases have been reported from Japan where cataract surgery and EDTA chelation were safely performed after introduction of biologics, achieving good visual improvement 6). Performing surgical intervention under controlled underlying disease is the most important factor determining long-term prognosis.
Advances in diagnostic imaging are also attracting attention. By combining three-dimensional evaluation of deposition layers using AS-OCT, corneal density analysis using Scheimpflug imaging, and time-series comparison of topographic indices, refinement of treatment indications and laser irradiation profiles is expected 1). In addition, clinical application of biomarkers (tear inflammatory cytokines, serum calcium-phosphorus product) to stratify recurrence risk derived from underlying diseases is a future challenge. Ensuring multidisciplinary collaboration (rheumatology, nephrology, endocrinology) at each stage of clinical practice is key to suppressing recurrence and preserving visual function.
Passidomo F, Addabbo G, Pignatelli F, Niro A, Buonamassa R. Combined Topography-Guided Trans-Epithelial PRK and PTK for Treatment of Calcific Band Keratopathy Unresponsive to EDTA Chelation Therapy. International medical case reports journal. 2025;18:187-194. doi:10.2147/IMCRJ.S493245. PMID:39896888; PMCID:PMC11784368.
Abusayf MM, Tobaigy MF. Blood tubes potassium ethylenediaminetetraacetic acid in comparison to calcium disodium ethylenediaminetetraacetic acid and disodium ethylenediaminetetraacetic acid for calcific band keratopathy. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2025;39(4):407-409. doi:10.4103/sjopt.sjopt_97_24. PMID:41367839; PMCID:PMC12685252.
Narvaez J, Chang M, Ing J, De Chance D, Narvaez JJ. Simplified, Readily Available Method for the Treatment of Band Keratopathy With Ethylenediaminetetraacetic Acid. Cornea. 2021;40(10):1360-1362. doi:10.1097/ICO.0000000000002635. PMID:34481414; PMCID:PMC8423137.
American Academy of Ophthalmology Corneal/External Disease PPP Panel. Corneal Edema and Opacification Preferred Practice Pattern. Ophthalmology. 2024.
Markoulli M, Ahmad S, Engel L, et al. TFOS Lifestyle: Impact of the natural, built, and social environments on the ocular surface. Ocul Surf. 2023;29:226-271.
Najjar DM, Cohen EJ, Rapuano CJ, Laibson PR. EDTA chelation for calcific band keratopathy: results and long-term follow-up. American journal of ophthalmology. 2004;137(6):1056-64. doi:10.1016/j.ajo.2004.01.036. PMID:15183790.
O’Brart DP, Gartry DS, Lohmann CP, Patmore AL, Kerr Muir MG, Marshall J. Treatment of band keratopathy by excimer laser phototherapeutic keratectomy: surgical techniques and long term follow up. The British journal of ophthalmology. 1993;77(11):702-8. doi:10.1136/bjo.77.11.702. PMID:8280683; PMCID:PMC504628.
Porter R, Crombie AL. Corneal and conjunctival calcification in chronic renal failure. Br J Ophthalmol. 1973;57(5):339-343.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.