The corneal epithelium is a stratified squamous epithelium that is completely renewed every 3 to 10 days. The stem cells that support this continuous regeneration reside in the limbus, the border between the cornea and conjunctiva. The palisades of Vogt (POV) described by Vogt in 1921 serve as the niche (microenvironment) for these stem cells1).
Limbal stem cell deficiency (LSCD) is a condition in which these stem cells are congenitally or acquiredly lost or become dysfunctional. When the self-renewal capacity of the corneal epithelium is lost, conjunctival epithelium invades the cornea, a process called conjunctivalization. Conjunctivalization leads to superficial neovascularization and corneal opacity, resulting in visual impairment.
The limbus also functions as a barrier preventing vascular invasion from the conjunctiva into the cornea. When this barrier breaks down, corneal transparency is lost. LSCD presents with varying severity, from partial (incomplete conjunctivalization) to total (complete conjunctivalization)1). It is believed that if as little as 7% of limbal stem cells remain, corneal epithelial reconstruction is possible with modern surgical techniques1).
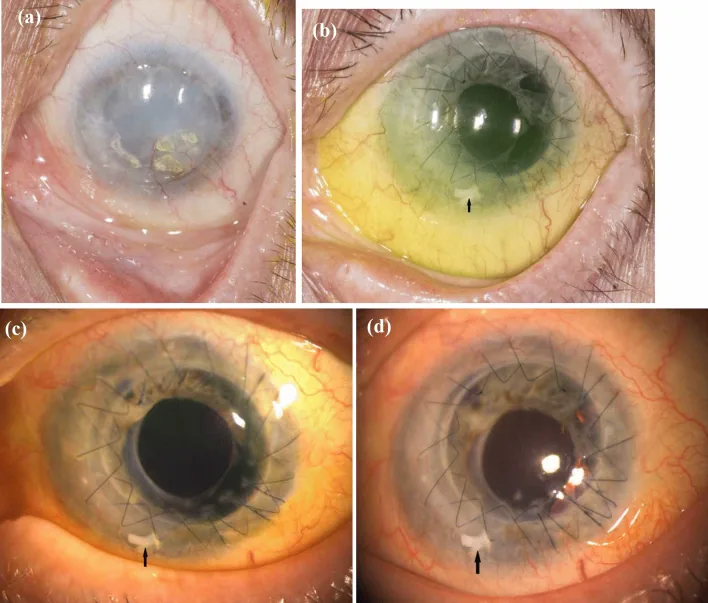
Anja Viestenz, Christiane Kesper, Thomas Hammer, Joana Heinzelmann, et al. ALT (allogeneic limbal transplantation): a new surgical technique for limbal stem cell deficiency 2022 Aug 19 Int Ophthalmol. 2022 Aug 19; 42(12):3749-3762 Figure 3. PMCID: PMC9617846. License: CC BY.
a shows preoperative corneal opacity and severe vascular invasion. b to d show postoperative progress, with surface epithelialization and recovery of transparency, and limbal grafts indicated by arrows.
The main complaints are eye pain and decreased vision due to recurrent epithelial erosion. Foreign body sensation, contact lens intolerance, photophobia, and tearing are also common. Infectious keratitis is likely to complicate due to disruption of the epithelial barrier.
Slit-lamp microscopy reveals the following findings in stages 1).
Mild: Whorl-epitheliopathy on fluorescein staining. Epithelial thinning from the limbus toward the center.
Moderate: Appearance of superficial neovascularization and peripheral pannus.
Severe: 360-degree conjunctivalization of the cornea, stromal neovascularization, corneal opacity/scarring. May lead to corneal perforation.
The global consensus published by the Cornea Society in 2019 proposes a clinical staging classification based on the extent of limbal involvement, corneal surface involvement, and impact on the visual axis 1).
POV is normally present around the entire limbus (especially easy to observe superiorly and inferiorly). In LSCD, POV disappears. However, POV may be difficult to observe even in normal individuals under 10 years or over 70 years of age.
In a 14-year epidemiological survey of 738 eyes at a tertiary facility, the causes were aniridia 30.9%, chemical/thermal burns 20.6%, CL 16.8%, and Stevens-Johnson syndrome 10.4%1).
Mehta et al. reported a case of a 56-year-old man who developed bilateral LSCD and extensive symblepharon 57 months after starting dupilumab. It was thought that goblet cell depletion due to IL-4/IL-13 signaling inhibition caused ocular surface inflammation, and chronic inflammation exhausted limbal stem cells.3)
Schumaier et al. reported a case of a 65-year-old man who developed bilateral LSCD-like findings and left corneal perforation 2 months after starting durvalumab for non-small cell lung cancer. The cornea highly expresses PD-L1, and inhibition of the PD-1/PD-L1 pathway may have triggered autoimmune keratitis. Conjunctival inflammation resolved after discontinuation of durvalumab.5)
QCan contact lenses cause LSCD?
A
Long-term contact lens wear can cause LSCD. This is especially common with soft contact lenses, with reports indicating that approximately 2–5% of contact lens wearers develop LSCD. The average duration of lens wear before onset of LSCD is 14–17 years. Mechanical irritation, hypoxic environment, and preservatives in lens solutions are thought to damage limbal stem cells.
Cultured oral mucosal epithelial transplantation (COMET): For bilateral LSCD, autologous oral mucosa is used as a substitute.4)
Keratoprosthesis (KPro): A last resort for severe total LSCD.
Cultured corneal epithelial transplantation (a regenerative medicine originating in Japan) and amniotic membrane transplantation are also used. In cases with severe inflammation such as SJS, mitomycin C may be used to suppress fibroblasts.
Booranapong et al. performed cultured oral mucosal epithelial sheet transplantation in 3 cases of chemical burn and 3 cases of Stevens-Johnson syndrome in Thailand. Two cases of chemical burn achieved excellent evaluation after 1 year, but the Stevens-Johnson syndrome cases had poor results because the oral mucosa itself was damaged, leading to low cell survival.4)
QCan't it be cured with corneal transplantation alone?
A
Corneal transplantation alone does not cure LSCD. What is provided in corneal transplantation is corneal stroma and endothelium, not corneal epithelial stem cells. After transplantation, the stem cell deficiency persists, and conjunctivalization and corneal opacity progress again, leading to graft failure. First, perform surgery to replenish limbal stem cells to stabilize the corneal surface, and then perform corneal transplantation in a second stage if needed.
Corneal epithelial stem cells are located in the basal cell layer of the palisades of Vogt (POV). Pigmentation of the POV protects stem cells from ultraviolet light. Stem cells migrate centripetally toward the center of the cornea as basal cells, move toward the surface while differentiating, and eventually shed.1)
Stem cell niche environment: Limbal stem cells require nutrient supply from the extra-corneal stromal vasculature, so they are located in the peripheral region near blood vessels. The cornea is avascular to maintain transparency, and stem cells exist in this transitional zone.
Mechanism of LSCD:
Damage to the limbal epithelium (chemical burns, inflammation, mechanical irritation, etc.)
Disruption of the stem cell niche microenvironment (inflammatory cytokines, matrix metalloproteinases)
Decrease in stem cells → reduced regenerative capacity of the corneal epithelium
Conjunctival epithelium invades the cornea (conjunctivalization)
Progression of superficial neovascularization, corneal opacity, and scarring
Limbal stem cells not only repopulate the corneal epithelium but also function as a barrier preventing vascular invasion from the conjunctiva. When this barrier function is lost, conjunctivalization and neovascularization occur, and corneal transparency is irreversibly compromised.
In partial LSCD, the remaining healthy limbus supplies corneal epithelium, so the prognosis is relatively good if the affected area is limited. In total LSCD, surgical intervention is essential.
LSCD due to novel drugs: LSCD caused by new biologic agents such as immune checkpoint inhibitors and dupilumab has been reported3)5). It has been proposed that dupilumab reduces goblet cells via IL-4/IL-13 inhibition, leading to chronic ocular surface inflammation and LSCD3). Durvalumab may disrupt corneal immune privilege by inhibiting PD-L1, potentially triggering autoimmune keratitis5).
New causes reported: Elmansouri et al. reported the first case of LSCD in a 10-year-old child following chickenpox6). Awareness of LSCD due to viral infection is increasing.
Regenerative medicine using oral mucosal epithelium: Cultured oral mucosal epithelial sheet transplantation (COMET) and SOMET are promising options for bilateral LSCD when limbal donors are unavailable4). Since autologous tissue is used, immunosuppression is unnecessary, and SOMET, which does not require cell culture infrastructure, can be performed in resource-limited settings.
Corneal epithelial regeneration using iPS cells: The use of iPS cells (induced pluripotent stem cells) is expected to solve the problems of donor shortage and rejection. In addition to autologous iPS cells, the use of allogeneic iPS cell banks with specific HLA types that have low immunogenicity is being considered. Differentiation of human iPS cells into corneal epithelial cells and production of cell sheets have been reported, and research is progressing toward clinical application as a new treatment option for bilateral LSCD.
Integration with gene therapy: Cultured limbal epithelial transplantation (CLET) allows gene transfer during in vitro culture. Combination with gene therapy is being considered for congenital LSCD such as epidermolysis bullosa. This is a treatment strategy not possible with CLAu or SLET, and is considered a unique clinical significance of CLET.
Advances in imaging diagnosis: Improvements in confocal microscopy and anterior segment OCT are enabling more precise early diagnosis and monitoring of treatment effects for LSCD1).
Application of genetic analysis: In hereditary LSCD such as aniridia, genetic sequencing may be used for prognosis prediction and treatment decision-making 1).
QDo immune checkpoint inhibitors also cause eye side effects?
A
Yes. Immune checkpoint inhibitors rarely cause ocular side effects. Uveitis and dry eye are relatively common, but severe cases have been reported leading to LSCD or corneal perforation. If eye symptoms (redness, pain, vision loss) appear after starting cancer treatment, it is important to promptly see an ophthalmologist.
Trief D, Rapuano CJ. Limbal stem cell deficiency: pathophysiology, clinical manifestations, diagnosis, and causes. Ann Eye Sci. 2023;8:13.
Basu S, Chodosh J. Conjunctival limbal autograft transplantation for limbal stem cell deficiency: a systematic review. Br J Ophthalmol. 2023 (247.full).
Mehta U, Farid M. Dupilumab Induced Limbal Stem Cell Deficiency. International medical case reports journal. 2021;14:275-278. doi:10.2147/IMCRJ.S308583. PMID:33981166; PMCID:PMC8107002.
Booranapong W, Kosrirukvongs P, Duangsa-Ard S, Kasetsinsombat K, Sa-Ngiamsuntorn K, Wongkajornsilp A. Transplantation of autologous cultivated oral mucosal epithelial sheets for limbal stem cell deficiency at Siriraj Hospital: a case series. Journal of medical case reports. 2022;16(1):298. doi:10.1186/s13256-022-03502-8. PMID:35922868; PMCID:PMC9351062.
Schumaier NP, Heidemann DG, Gupta C. Durvalumab-associated limbal stem cell deficiency and secondary corneal perforation. American journal of ophthalmology case reports. 2024;35:102074. doi:10.1016/j.ajoc.2024.102074. PMID:38975031; PMCID:PMC11225003.
Elmansouri O, Lemkhoudem A, Bezza H, Ait Lhaj H, Kriet M, Elasri F. Limbal stem cell deficiency: a dreaded complication of chickenpox in children. Oxford medical case reports. 2025;2025(5):omaf037. doi:10.1093/omcr/omaf037. PMID:40443855; PMCID:PMC12118088.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.