Cornea verticillata is a finding in which deposits appear in a whorl-like pattern in the basal epithelial layer of the cornea. It is also called vortex keratopathy, whorl keratopathy, or Fleischer vortex. “Verticillata” is Latin for “whorl.”
It is usually asymptomatic and is often discovered incidentally during slit-lamp examination. It results from the accumulation of drugs, metabolic substrates, or disease byproducts in the lysosomes of the corneal basal epithelium. Amiodarone and Fabry disease are the most common causes.
QDoes cornea verticillata affect vision?
A
Cornea verticillata usually does not affect vision. Rarely, patients may see a blue-green ring or halos, but most patients have no symptoms. In drug-induced cases, it typically disappears after discontinuation of the causative drug. The presence of cornea verticillata itself does not require a change in medication, but evaluation of the underlying disease (especially Fabry disease) is important.
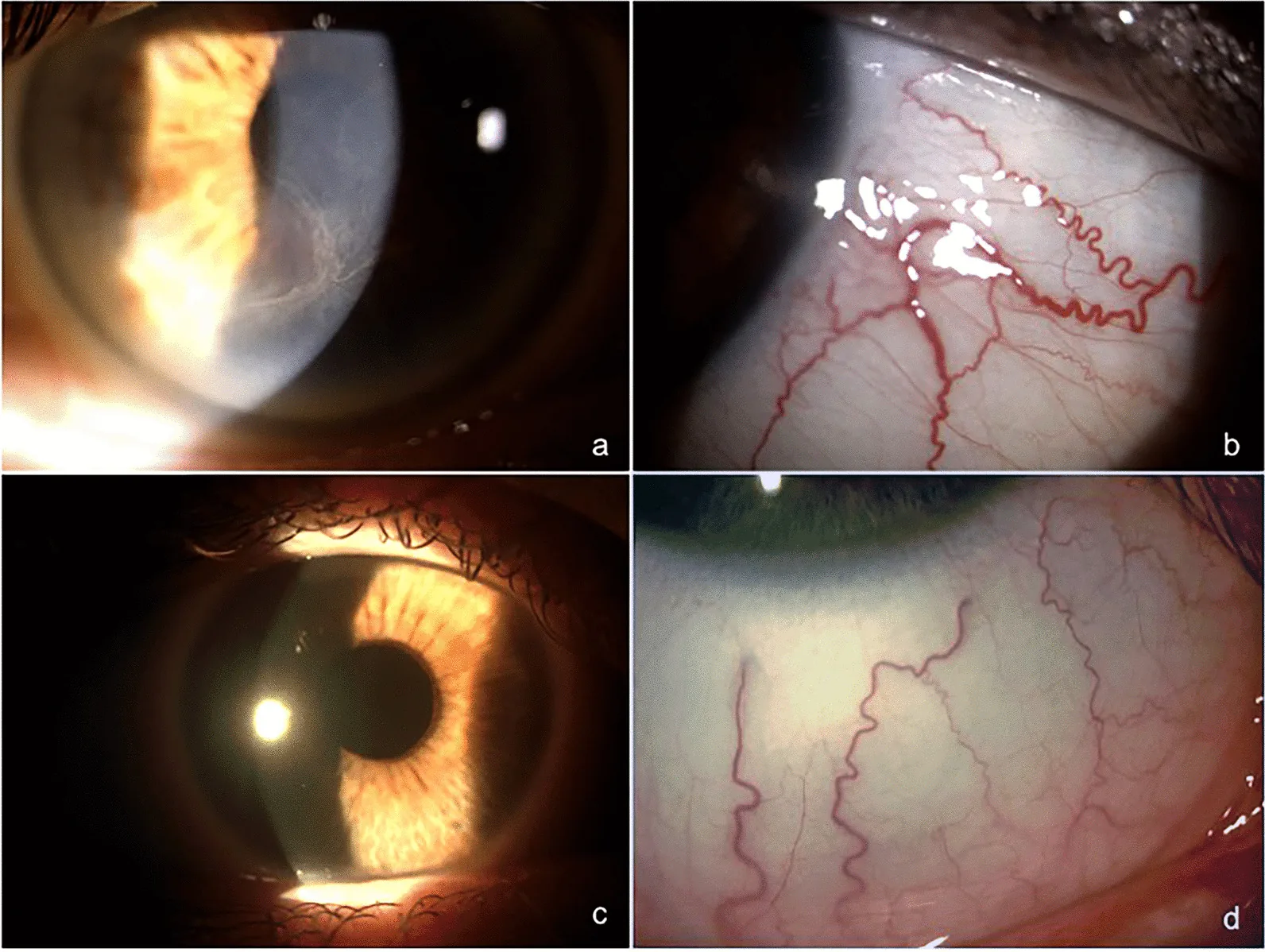
Marco Marenco, Marco Segatto, Marta Sacchetti, Pietro Mangiantini, et al. Autophagy-lysosome pathway alteration in ocular surface manifestations in Fabry disease patients 2022 Jul 23 Orphanet J Rare Dis. 2022 Jul 23; 17:291 Figure 1. PMCID: PMC9308246. License: CC BY.
Ophthalmologic microscope images showing cornea verticillata and conjunctival vessel tortuosity in a Fabry disease patient. Image a shows cornea verticillata, image b shows conjunctival vessel tortuosity. Image c shows a healthy cornea, image d shows healthy conjunctival vessels.
Most patients with cornea verticillata are asymptomatic. Rarely, they may see halos around lights or complain of blurred vision. In netharsuljil-induced cases, glare and blurred vision have been reported2).
Slit-lamp microscopy reveals fine golden-brown to gray whorl-like opacities in the corneal basal epithelium. The opacities typically spread in a branching pattern centered on the lower cornea. They are not stained with fluorescein and are almost always bilateral.
Slight differences in opacity patterns may be seen between drug-induced cases and Fabry disease. Drug-induced cases tend to appear as horizontal lines with fine branching at the ends. Fabry disease presents a curved pattern forming whorls before straightening in the peripheral cornea.
In amiodarone keratopathy, brown whorl-like deposits are seen in the deep epithelium slightly below the central cornea, classified as grade I to IV by the Orlando classification. At high doses (400 mg/day), they appear in nearly 100% of cases.
Other non-drug causes include multiple myeloma, generalized gangliosidosis, multiple sulfatase deficiency, and Lisch corneal dystrophy.
QWhich medications cause vortex keratopathy?
A
Typical drugs that cause vortex keratopathy include amiodarone (antiarrhythmic), hydroxychloroquine/chloroquine (antimalarials), and indomethacin (NSAID). Recently, netarsudil (ROCK inhibitor), a glaucoma medication, has also been reported to cause vortex keratopathy. These drugs share cationic and amphiphilic properties and accumulate in the lysosomes of the corneal basal epithelium. Discontinuation of the causative drug is expected to lead to improvement.
Scleral scatter method clearly visualizes the whorl-like opacities on the corneal epithelial surface. Retroillumination or use of a cobalt blue filter is also useful for delineating the opacity pattern.
Confocal laser scanning microscopy is useful for differentiating between drug-induced and Fabry disease. In Fabry disease, characteristic hyperreflective deposits are observed in the corneal epithelium, stroma, and limbal region, which correlate with disease severity and systemic involvement.
If Fabry disease is suspected from vortex keratopathy, the following examinations are performed. In males, enzyme activity is a reliable indicator, but in females, due to lyonization (X-chromosome inactivation), enzyme activity may be normal, making genetic testing essential1).
Measurement of α-galactosidase A activity (DBS method)
Measurement of plasma Lyso-Gb3 (globotriaosylsphingosine)
QWhen should Fabry disease be suspected from vortex keratopathy?
A
If vortex keratopathy is present without a history of medication, Fabry disease is suspected. It is strongly suspected especially when vortex keratopathy accompanies vascular events (cerebral infarction, CRAO) in young patients. In males, diagnosis can be made by decreased α-galactosidase A activity, but in female carriers, enzyme activity may be normal, so GLA genetic testing is necessary. Early diagnosis and treatment of Fabry disease affect prognosis, so detection of vortex keratopathy is an important opportunity.
Treatment for vortex keratopathy itself is usually unnecessary. The deposits do not significantly affect vision. If only vortex keratopathy is present, no change in medication regimen or further workup is needed.
Discontinuation of the causative drug leads to resolution of deposits. Vortex keratopathy and conjunctival pigmentation due to neltarsudil completely resolved 14 months after drug cessation2).
In vortex keratopathy due to intravitreal methotrexate, frequent artificial tears, loteprednol, topical folic acid (5 mg/mL), and oral folic acid led to complete resolution within 3 weeks4). Thorough irrigation of the corneal surface after intravitreal injection is useful for prevention4).
Patients using hydroxychloroquine, chloroquine, chlorpromazine, or tamoxifen are at risk of retinal toxicity. The presence of vortex keratopathy does not directly correlate with retinal toxicity, but regular monitoring with automated perimetry and SD-OCT is recommended.
Vortex keratopathy in Fabry disease is not a direct indication for enzyme replacement therapy (ERT), but ERT is administered for systemic management. A decrease in blood Lyso-Gb3 has been confirmed after starting ERT1). In one family, the mother’s Lyso-Gb3 decreased from 21.76 to 12.72 nmol/L and the son’s from 156.50 to 27.48 nmol/L after 6 months of ERT1).
The corneal epithelium migrates centripetally from the limbal stem cells toward the center. Limbal stem cells containing drugs or lipids migrate along this centripetal pathway, forming a vortex pattern.
Drug-Induced Mechanism
Common property: Cationic and amphiphilic drugs penetrate the lysosomes of the corneal basal epithelium.
Accumulation process: Drug-lipid complexes are resistant to enzymatic degradation and accumulate as deposits.
Amiodarone: Inhibits lysosomal phospholipase A2.
Netarsudil: Phospholipidosis in corneal epithelial cells is presumed to be the mechanism2).
Mechanism in Fabry Disease
Enzyme deficiency: Due to deficiency of α-galactosidase A
Accumulated substance: Glycosphingolipids (mainly Gb3) accumulate in lysosomes
Deposition site: Progressively accumulates in lysosomes of systemic tissues including the cornea
Gene: Mutation in the GLA gene. Over 1000 mutations have been reported1)
Mechanism of methotrexate-induced vortex keratopathy
Intravitreal methotrexate is thought to cause direct toxicity to limbal stem cells4). Drug leakage into the subconjunctival space after injection damages limbal stem cells, leading to transient limbal dysfunction and vortex keratopathy4). Because it is reversible, the damage is presumed to affect proliferating stem cells rather than the stem cell niche4).
Relationship with drug-induced corneal epithelial disorders
Vortex keratopathy appears as a morphology in which the corneal surface is covered by migration of superficial cells when increased shedding of corneal epithelium persists and cannot be compensated by basal cell proliferation alone. If this progresses, it can develop into persistent epithelial defects via epithelial crack lines.
Over 1000 mutations have been identified in the GLA gene of Fabry disease, and reports of novel mutations continue. In one study, a frameshift mutation c.484delT (p.W162Gfs*3) was reported for the first time as a cause of classic Fabry disease1). Another report confirmed the first case of Fabry disease in Malaysia, where vortex keratopathy led to the diagnosis3).
In addition to ROCK inhibitor-induced vortex keratopathy, a new report described the complication of conjunctival pigmentation2). Pigmentation must be differentiated from primary acquired melanosis, but its disappearance after drug discontinuation is a distinguishing feature2).
A case in which vortex keratopathy led to the discovery of Fabry disease in a young patient with CRAO5) highlights the importance of early detection by ophthalmologists.
Giacalone I, Ruzzi L, Anania M, Cuonzo M, Marsana EM, Mastrippolito S, et al. The Identification of a Novel Pathogenic Variant of the GLA Gene Associated with a Classic Phenotype of Anderson-Fabry Disease: A Clinical and Molecular Study. International journal of molecular sciences. 2025;26(2). doi:10.3390/ijms26020470. PMID:39859185; PMCID:PMC11764866.
Azargui S, Karanxha J, Oliver SC, Kahook MY, Capitena Young CE. Netarsudil-associated conjunctival pigmentation. American journal of ophthalmology case reports. 2025;38:102311. doi:10.1016/j.ajoc.2025.102311. PMID:40236508; PMCID:PMC11998109.
Tang ASO, Wong QY, Pao Lin Ting I, Selvesten P, Yeo ST, Chew LP, et al. First 2 Fabry Cases with Novel Mutation and Their Associated Clusters in Malaysia. The American journal of case reports. 2021;22:e932923. doi:10.12659/AJCR.932923. PMID:34354036; PMCID:PMC8351246.
Hasan N, Narde HK, Das AK, Chawla R. Unusual presentation of cornea verticillata with intravitreal methotrexate in a case of primary intraocular lymphoma. BMJ Case Rep. 2022;15:e246911.
Nakata D, Okada H, Shimada Y, Tanikawa A, Horiguchi M, Ito Y. A Case of Fabry Disease with Central Retinal Artery Occlusion. Case reports in ophthalmology. 2022;13(2):584-588. doi:10.1159/000524926. PMID:36160490; PMCID:PMC9459517.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.