Cornea farinata is a finding in which fine dust-like opacities appear just anterior to Descemet’s membrane in the deepest layer of the corneal stroma1). It was first described by Swiss ophthalmologist Arthur Vogt and is also called “floury cornea.”
It occurs bilaterally and progresses slowly with age. Since it does not affect vision, its clinical significance is limited. It is classified as a degeneration, not a corneal dystrophy. Reports in individuals under 40 are rare. In vivo confocal microscopy (IVCM) shows highly reflective particles within the cytoplasm of keratocytes in the deep corneal stroma1).
Similar deep corneal opacities are also observed in patients with X-linked ichthyosis (XLI) caused by mutations in the STS gene (Xp22.31) 2,3). They are found in 50% of patients and 25% of female carriers, appearing from early adulthood 2). In this case, it is not due to aging but results from steroid sulfatase deficiency and accumulation of cholesterol sulfate 3).
QDoes cornea farinata require treatment?
A
Cornea farinata usually does not require treatment. Since it is asymptomatic and does not affect vision, only observation is needed. However, it is important to differentiate it from conditions like Fuchs’ endothelial corneal dystrophy, which also presents with deep corneal opacities. Fuchs’ is accompanied by a decrease in corneal endothelial cell density, whereas in cornea farinata the corneal endothelium is normal.
Joobin Khadamy Ocular Manifestations Leading to the Diagnosis of Ichthyosis: A Case Report 2025 Mar 4 Cureus.; 17(3):e80023 Figure 2. PMCID: PMC11968076. License: CC BY.
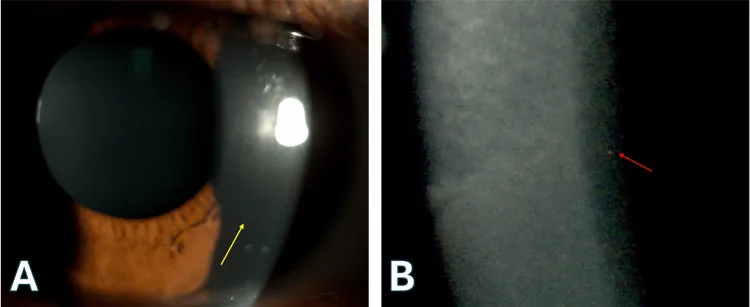
Image A is an eye photograph taken by slit-lamp microscopy, showing elevated corneal nerves (yellow arrows). Image B is a magnified view from the same slit-lamp microscopy, showing punctate opacities in the deep corneal stroma (red arrows). These findings are consistent with a diagnosis of cornea farinata.
Cornea farinata is usually asymptomatic. It does not cause decreased vision, eye pain, foreign body sensation, or photophobia. In many cases, it is discovered incidentally during slit-lamp examination.
On slit-lamp microscopy using retroillumination or specular reflection, fine gray-white to yellowish-brown granular deposits are seen on the posterior corneal surface. The opacities are densely distributed in the central to paracentral cornea and decrease toward the periphery. Individual deposits are extremely small and can be easily missed with direct slit-beam illumination.
The opacities are diffusely and uniformly distributed in the corneal stroma anterior to Descemet’s membrane. Descemet’s membrane, corneal epithelium, and endothelial cell layer are normal. Corneal thickness is within normal range. Specular microscopy shows normal morphology and density of corneal endothelial cells.
The greatest risk factor is aging. It is commonly observed in elderly individuals and progresses slowly, but rarely becomes clinically significant. Reports in individuals under 40 years of age are rare.
Steroid sulfatase deficiency due to mutations in the STS gene (Xp22.31) causes X-linked ichthyosis (XLI). In XLI patients, cholesterol sulfate accumulates in the deep corneal stroma, leading to opacities similar to corneal farinata. At least six different mutations in the STS gene have been reported, and the type of mutation affects the expression and function of the steroid sulfatase enzyme, resulting in various phenotypes.
Other differential diagnoses include fleck corneal dystrophy, deep filiform dystrophy, and posterior punctiform dystrophy. All present with opacities in the deep corneal layer, but the morphology and distribution of opacities differ.
Differentiation from Fuchs endothelial corneal dystrophy may be difficult with slit-lamp microscopy alone, and specular microscopy is necessary. In corneal farinata, no abnormalities are observed in the corneal endothelium.
QWhat is the difference from Fuchs endothelial corneal dystrophy?
A
Both corneal farinata and Fuchs endothelial corneal dystrophy show findings in the deep corneal layers, but the decisive difference is the condition of the corneal endothelium. In corneal farinata, specular microscopy shows normal morphology and density of corneal endothelial cells, whereas in Fuchs, guttae on Descemet’s membrane and decreased endothelial cell density are observed. Fuchs progresses to corneal edema and bullous keratopathy, but corneal farinata does not affect vision.
With aging, lipofuscin-like inclusions accumulate in the cytoplasm of keratocytes in the corneal stroma just anterior to Descemet’s membrane. Histopathologically, they are observed as intracytoplasmic vacuoles containing lipofuscin-like inclusions and may cause abnormal enlargement of keratocytes.
Lipofuscin is a product of lipid peroxidation due to intracellular oxidative stress, and its accumulation progresses with age. The mechanism of selective accumulation in deep stromal keratocytes is not fully understood.
Steroid sulfatase deficiency due to STS gene mutation causes impaired metabolism of cholesterol sulfate. Accumulated cholesterol sulfate deposits in keratocytes, presenting a dust-like opacity similar to age-related corneal farinata. STS is localized in the endoplasmic reticulum and may be involved in the formation of lipofuscin-like deposits seen histopathologically.
Corneal deposits in XLI tend to appear at a younger age than age-related changes and are more widely distributed. It has been suggested that XLI and age-related corneal fariniform degeneration may share a common pathophysiological basis, but further research is needed for detailed elucidation 3).
Kobayashi A, Ohkubo S, Tagawa S, Uchiyama K, Sugiyama K. In vivo confocal microscopy in the patients with cornea farinata. Cornea. 2003;22(6):578-581.
Costagliola C, Fabbrocini G, Illiano GM, Scibelli G, Delfino M. Ocular findings in X-linked ichthyosis: a survey on 38 cases. Ophthalmologica. Journal international d’ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 1991;202(3):152-5. doi:10.1159/000310197. PMID:1923309.
Hung C, Ayabe RI, Wang C, Frausto RF, Aldave AJ. Pre-Descemet corneal dystrophy and X-linked ichthyosis associated with deletion of Xp22.31 containing the STS gene. Cornea. 2013;32(9):1283-7. doi:10.1097/ICO.0b013e318298e176. PMID:23807007; PMCID:PMC3740086.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.