Bullous keratopathy is a condition in which irreversible edema of the corneal stroma and epithelium occurs due to damage to corneal endothelial cells, and as it progresses, blisters (bullae) form under the epithelium. The main cause of vision loss is stromal edema, but pain results from the rupture of epithelial bullae.
The corneal endothelium maintains a constant water content and thickness of the corneal stroma through its pump function and barrier function with selective permeability. When the endothelial cell density falls below 400–500 cells/mm², the pump function becomes decompensated, leading to stromal edema, and with further progression, epithelial edema and bullae form. Because corneal endothelial cells do not divide in the anterior chamber, the damage is irreversible.
Pseudophakic bullous keratopathy (PBK) occurs in 1–2% of patients who have undergone cataract surgery, and it typically becomes apparent between 8 months and 7 years after surgery 1). With advances in cataract surgery techniques, the incidence has been decreasing, but it remains a major indication for corneal transplantation along with Fuchs endothelial corneal dystrophy4,8).
Corneal endothelial cell density physiologically decreases with age. In newborns, it is 3,500–4,000 cells/mm²; in the 20s, about 2,700 cells/mm²; and in those aged 70 and older, it decreases to an average of about 2,200 cells/mm². The normal physiological rate of decline is 0.5% per year, but after cataract surgery it accelerates to about 2% per year, and after glaucoma surgery to about 10% per year.
Fuchs endothelial corneal dystrophy has an autosomal dominant inheritance pattern and is more common in women, with a female-to-male ratio of about 4:1 4). It has been reported to be less common in Japanese people compared to Caucasians and Blacks, but cornea guttata, a precursor condition, is observed in 1.2% of preoperative cataract patients, and with increasing longevity, an increasing trend has been noted in Japan.
Bullous keratopathy is one of the major causes of visual impairment due to corneal disease and is a leading indication for corneal transplantation worldwide. Since cataract surgery is the most commonly performed ophthalmic surgery globally, pseudophakic bullous keratopathy is also important from a public health perspective. The incidence has been decreasing year by year due to less invasive surgical techniques, improved viscoelastic materials, and advances in ultrasound energy reduction technology, but it has not been completely eliminated. In recent years, the increase in cataract surgery among very elderly patients and the presence of pre-existing Fuchs endothelial corneal dystrophy carriers have been re-recognized as risk factors.
The major indications for corneal transplantation worldwide are Fuchs endothelial corneal dystrophy and pseudophakic bullous keratopathy 8). In Japan, there is a chronic shortage of corneal donors, and a high dependence on overseas donors is characteristic. According to recent domestic statistics, bullous keratopathy (including pseudophakic and aphakic types) accounts for about 40–50% of all corneal transplants. Although the absolute number has decreased with the less invasive nature of cataract surgery, it remains a major indication for corneal transplantation. Bullous keratopathy after laser iridotomy (LI) was once common in Japan but has decreased with the shift to prophylactic cataract surgery.
QDoes bullous keratopathy heal on its own?
A
No, bullous keratopathy is a condition caused by irreversible damage to corneal endothelial cells and does not heal spontaneously. Since human corneal endothelial cells have extremely limited capacity for division and regeneration, once lost, they cannot be restored. The definitive treatment is corneal endothelial transplantation, and in recent years, regenerative medicine using cultured corneal endothelial cells has been advancing toward practical application.
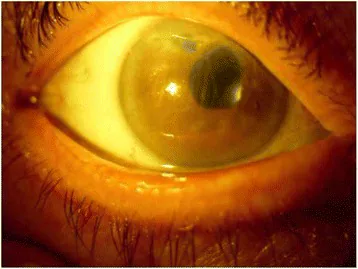
Pacella F, Agostinelli E, Carlesimo SC, et al. J Med Case Rep. 2016;10:282. Figure 2. PMCID: PMC5062904. License: CC BY.
The entire cornea shows diffuse whitish opacity, making the pupillary margin and iris details difficult to see. This is a clinical image of a severe case where opacity due to stromal edema extends throughout the anterior segment.
The subjective symptoms of bullous keratopathy vary depending on the degree of edema and the affected layer.
Visual impairment: This is the most prominent symptom. In the early stage, a characteristic diurnal variation is observed, with vision worsening in the morning and improving during the day. During eyelid closure, tear evaporation decreases, leading to accumulation of edema, which gradually reduces after opening the eyes due to evaporation. As the condition progresses, irreversible persistent visual impairment occurs.
Eye pain: Occurs with rupture of subepithelial bullae. In severe cases, the pain can be intolerable and cause nighttime awakening.
Foreign body sensation: Caused by epithelial defects due to bulla rupture or irregularity of the corneal surface.
Photophobia and tearing: Result from optical irregularity of the corneal surface and trigeminal nerve stimulation.
Slow onset: Progresses gradually over weeks to months, so patients may adapt relatively well.
Corneal stromal edema: Presents as ground-glass corneal opacity. Corneal thickness increases markedly, sometimes exceeding 800 μm.
Descemet’s membrane folds: Folds form on the posterior corneal surface due to endothelial dysfunction. This is an important indicator of endothelial damage.
Subepithelial bullae: In advanced cases, giant bullae form, and rupture leads to epithelial defects and pain.
Stromal scarring and vascularization: Chronicity leads to peripheral vascularization and scar opacification, contributing to vision loss.
Characteristic findings by cause
Fuchs endothelial corneal dystrophy: Begins with central guttae, progressing to a beaten-metal appearance. Observed as dark spots on specular microscopy.
Pseudophakic: Check the type and position of the intraocular lens. Anterior chamber IOLs carry high risk; also evaluate the endothelial status of the fellow eye.
On slit-lamp examination, if stromal edema without inflammatory signs is observed, endothelial dysfunction should be considered first. Stromal edema after intraocular surgery is usually most prominent near the wound site, and stromal edema also appears around infiltrates in infectious keratitis. On fluorescein staining, epithelial bullae appear as dark spots.
Signs suggestive of corneal endothelial abnormality include gray-white or brownish droplets observed on the endothelial surface near the central cornea. When droplets enlarge and coalesce, they show a characteristic beaten-metal appearance, seen as dark spots on specular reflection or endothelial microscopy.
Epithelial edema stage: Formation of epithelial microcysts; photophobia and foreign body sensation increase.
Bulla formation stage: Subepithelial bullae form; severe eye pain and epithelial defects occur upon rupture.
Scarring stage: Chronic progression of subepithelial scarring, vascular invasion, and stromal opacity.
Treatment strategies differ at each stage. Up to the stromal edema stage, conservative treatment and medication may allow observation, but from the bullous stage onward, pain management and consideration of endothelial transplantation become necessary.
QWhy is vision worse in the morning?
A
When corneal endothelial function is reduced, tear evaporation decreases during eyelid closure (sleep), making corneal edema more likely to accumulate. During the day, tear evaporation draws water out of the cornea, reducing edema and improving vision. This pattern is known as a typical symptom of bullous keratopathy and early Fuchs endothelial corneal dystrophy.
Corneal endothelial cells do not divide or proliferate in vivo. Local damage is repaired by enlargement and migration of adjacent cells, but when the density falls below a certain level, irreversible decompensation occurs. The causes of bullous keratopathy are diverse: iatrogenic, degenerative, traumatic, inflammatory, and drug-induced. The most frequent are pseudophakic bullous keratopathy (PBK) and Fuchs endothelial corneal dystrophy.
Risk Factors for Pseudophakic Bullous Keratopathy (PBK)
Anterior chamberIOL (ACIOL) has been reported to cause PBK in approximately 14% of cases, which is higher risk than posterior chamber IOL3). The postoperative endothelial cell loss rate is about 2.5% per year, approximately 4 times faster than the normal 0.6% per year. A decrease of about 11% from preoperative levels at 5 years and about 18.7% at 10 years or more has been reported.
This is a bilateral progressive endothelial disease with autosomal dominant inheritance, characterized by guttae in the central cornea that gradually spread to the periphery4). It usually does not cause symptoms before age 50 and progresses slowly. As it advances, both barrier and pump functions of the endothelium decline, leading to bullous keratopathy.
After laser iridotomy: Argon laser energy directly damages endothelial cells. Japanese individuals often have narrow angles, and endothelial cell loss after this procedure is a concern.
After corneal cross-linking (CXL): Late-onset corneal edema has been reported as a rare complication. Vandevenne et al. reported a case of microcystic corneal edema 4 months after customized cross-linking for progressive keratoconus, with endothelial cell density decreasing by 37% from 2,414 to 1,514 cells/mm², but resolving spontaneously within 1 month5).
Drug-induced: Amantadine (permanent damage with long-term use), chlorpromazine, gold preparations, ROCK inhibitor netarsudil. Chu et al. reported a 79-year-old woman who developed severe edema with corneal thickness increasing from 557 to 808 μm 5 days after starting netarsudil; complete recovery occurred after discontinuation and treatment with hypertonic saline and steroid eye drops over 4 months6).
Toxic anterior segment syndrome (TASS): Non-infectious inflammation due to toxic irrigating solutions or inadvertent intraocular injection of drugs. Arici et al. reported a case of diffuse corneal edema after uneventful pterygium surgery, suspected to be due to corneal endothelial toxicity from PVP-I. It resolved within 2 weeks with intensive dexamethasone eye drops, but endothelial cell density decreased to 1,001 cells/mm² after 1 year7).
Soemmering ring degradation: 20–30 years after cataract surgery, calcified particles from retained lens material may detach and deposit on the corneal endothelium.
Trauma/forceps delivery: Rupture of Descemet’s membrane can progress to endothelial dysfunction. Damage at birth may become apparent over a long course.
ICE syndrome (iridocorneal endothelial syndrome): Unilateral, with iris atrophy, pupillary distortion, and peripheral anterior synechiae; abnormal endothelial cells spread across the posterior cornea causing edema.
Secondary glaucoma: Chronic elevated intraocular pressure increases the load on the endothelial pump and accelerates endothelial cell loss over time.
Long-term contact lens wear: Chronic hypoxia causes endothelial cell morphological abnormalities (polymegethism, pleomorphism), increasing the risk of future decompensation.
Diabetes: Contributes to decreased endothelial cell function and increased risk of postoperative complications.
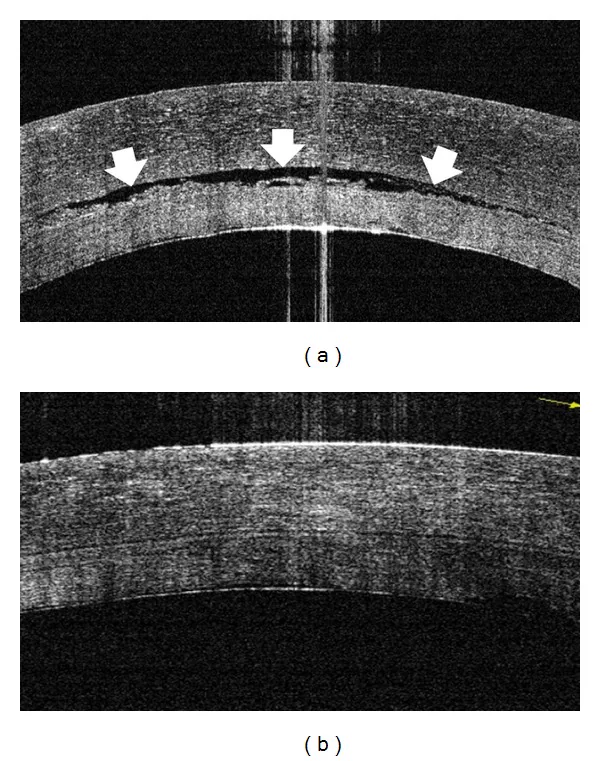
Miyakoshi A, Ozaki H, Otsuka M, et al. Efficacy of Intraoperative Anterior Segment Optical Coherence Tomography during Descemet’s Stripping Automated Endothelial Keratoplasty. ISRN Ophthalmol. 2014;2014:562062. Figure 4. PMID: 24634787; PMCID: PMC3929380; DOI: 10.1155/2014/562062. License: CC BY.
Anterior segment OCT compares subepithelial fluid accumulation and corneal edema before and after improvement. This is a representative image showing the layered structural changes in bullous keratopathy.
The diagnosis of bullous keratopathy is based on clinical findings, with supplementary tests evaluating endothelial function and the degree of edema.
This is the most basic examination. The extent and depth of corneal opacity are assessed using retroillumination, and the spread of epithelial edema is confirmed using scleral scatter. With specular reflection, a beaten-metal appearance of the endothelium can be observed in Fuchs-related cases.
The edema pattern is useful for estimating the cause. Diffuse edema suggests TASS or drug toxicity, localized edema suggests Descemet’s membrane detachment or instrument contact, and disciform edema suggests herpetic corneal endotheliitis. In corneal transplant eyes, sectoral edema and corneal endothelial deposits (Khodadoust line) suggest rejection.
This is the central examination for evaluating corneal endothelial cell density and morphology.
Parameter
Normal Value
Abnormal Value
Cell Density
2,200–4,000 cells/mm² depending on age
Maintaining transparency is difficult below 500 cells/mm²
CV value (coefficient of variation)
0.2–0.3
0.35 or higher
Hexagonal cell rate
60–70%
50% or less
In mild cases, it is useful for preoperative evaluation, but imaging becomes difficult in cases with severe edema. In such cases, contact specular microscopy or confocal microscopy is useful.
It is essential for quantitative evaluation of edema. Ultrasound pachymetry is a rapid and standard examination, while anterior segment OCT and Scheimpflug imaging allow non-contact measurement of multiple sites 9).
It can visualize each layer of the cornea at high resolution, allowing detailed evaluation of the extent of subepithelial bullae, stromal thickening, and Descemet membrane abnormalities. It is useful for identifying structural abnormalities that are difficult to confirm with slit-lamp examination 9). In particular, it can be applied widely, including postoperative evaluation, detection of Descemet membrane detachment, assessment of the extent of epithelial edema, and confirmation of graft adhesion. Anterior segment OCT is non-contact, imposes little burden on the patient, and is suitable for longitudinal observation.
In cases of severe corneal edema where evaluation with specular microscopy is difficult, confocal microscopy is useful. It allows direct observation of the corneal endothelial cell morphology and assessment of cell density and pleomorphism. In research settings, it is also used to observe the nerve plexus, keratocytes, and immune cells.
Age-related changes in endothelial cell density and preoperative evaluation
In elderly patients undergoing cataract surgery, in addition to age-related natural decline, coexisting systemic diseases and a history of previous ocular surgery or trauma affect the state of endothelial cells. Based on specular microscopy findings obtained preoperatively, surgical prognosis and the risk of developing bullous keratopathy are estimated. Particularly in cases with endothelial cell density ≤1,000 cells/mm², CV ≥0.4, and hexagonal cell rate <40%, the risk of postoperative decompensation is high, and surgical modifications such as generous use of viscoelastic materials, minimization of ultrasound energy, and management of hard nuclei are required.
Treatment of bullous keratopathy combines medical and surgical approaches depending on the reversibility of endothelial damage and visual requirements.
Treatment is based on four pillars: “removal of cause,” “preservation and recovery of endothelial function,” “reduction of edema and pain,” and “restoration of visual function.” In the reversible stage of endothelial damage (inflammatory, drug-induced, transient postoperative), resolution of the cause can lead to improvement of edema. In the irreversible stage, symptomatic management with conservative treatment and radical treatment with surgery are the mainstays.
This is performed as a bridge to endothelial transplantation or as symptomatic therapy for cases where surgery is difficult.
5% sodium chloride eye drops / 6% sodium chloride eye ointment: Makes the tear film hypertonic to osmotically draw water out of the cornea. Applying ointment before bedtime is useful for suppressing overnight edema accumulation. The effect is limited to epithelial edema and has little effect on stromal edema.
Therapeutic soft contact lens (BCL): Useful for relieving pain associated with rupture of epithelial bullae. Because of the risk of infectious keratitis, regular follow-up and prophylactic antibiotic eye drops are recommended.
Steroid eye drops: Used when inflammation is involved. May enhance Na⁺/K⁺-ATPase pump activity in the endothelium.
Intraocular pressure-lowering drugs: Used when elevated intraocular pressure is involved. However, topical administration of carbonic anhydrase inhibitors is not first-line in endothelial dysfunction because of concerns about interference with endothelial pump function. Prostaglandin analogs require caution as they may induce inflammation.
Hair dryer method: A simple method to accelerate daytime visual improvement by directing warm air from a hair dryer toward the corneal surface in the morning to promote evaporation.
Rho-associated coiled-coil forming kinase (ROCK) inhibitors promote corneal endothelial cell proliferation, migration, and adhesion, and suppress apoptosis. Erdinest et al. reported that in three cases of PBK that did not respond to conventional conservative treatment, administration of ripasudil 0.4% eye drops three times daily for 3–11 months resulted in decreased central corneal thickness and improved corrected visual acuity in all cases, avoiding corneal transplantation 10). In case 3, after 11 months of treatment, stromal opacity completely disappeared, central corneal thickness decreased from 582 μm to 540 μm, and visual acuity improved from 0.3 logMAR to 0.04 logMAR.
Furthermore, perioperative administration of ripasudil has been reported to result in a 12-month endothelial cell loss rate of 4.5% in the ripasudil group versus 12.8% in the control group after cataract surgery in high-risk eyes, suggesting potential prophylactic use 1).
DSAEK: Transplantation of the donor corneal endothelial layer and 50–100 μm of posterior stroma. Sutureless, with little induced astigmatism and excellent resistance to trauma.
Ultrathin DSAEK (UT-DSAEK): A technique that thins the graft to less than 130 μm, aiming for visual outcomes close to DMEK.
DMEK: Selective transplantation of only Descemet’s membrane and the endothelial cell layer. Faster and better visual recovery, with a lower rejection rate.
Indications: In principle, the eye should be pseudophakic, and the case should not have severe stromal opacity. Aniridia or extensive anterior synechiae limit the indication.
Penetrating Keratoplasty (PK)
Indications: Selected for cases with severe stromal scarring or vascular invasion where endothelial transplantation alone is unlikely to improve vision.
Features: The risk of postoperative rejection is higher than with endothelial transplantation, requiring long-term management with steroid eye drops.
Cautions: Postoperative corneal strength is reduced, and wound dehiscence can occur with blunt trauma.
A meta-analysis by Sela et al. (8 studies including 3 RCTs, 2 fellow-eye studies, and 3 cohort studies; 376 eyes: 187 DMEK, 189 UT-DSAEK) showed that logMAR BCVA at 12 months was significantly better in the DMEK group (mean difference −0.06, 95% CI −0.10 to −0.02)8). However, the frequency of requiring air reinjection (rebubbling) was 19.79% for DMEK and 8.99% for UT-DSAEK, significantly higher in the DMEK group (OR 2.76, 95% CI 1.46–5.22)8). Interestingly, when DSAEK graft thickness was less than 70 μm, no significant difference in BCVA was observed, suggesting that thinning may reduce the gap between the two procedures8).
Cases in which edema does not improve even after 6 months postoperatively are judged as endothelial decompensation and are indicated for corneal endothelial transplantation 9). DSAEK can also be performed in complex eyes such as those with microcornea or retained ACIOL, and good visual recovery without IOL exchange has been reported 3).
Selection of surgical method and postoperative management
The choice between DMEK and DSAEK is based on the presence of complex ocular conditions, surgeon experience, expected visual prognosis, and postoperative management system. In complex eyes (extensive iris defects, anterior chamberIOL, history of vitrectomy, glaucoma tube insertion, aphakia), graft unfolding and positioning are difficult, so DSAEK (or ultrathin DSAEK) is safer 3,8). On the other hand, in uncomplicated cases, DMEK offers advantages of earlier visual recovery and lower rejection rate 9).
In postoperative management, anterior chamber tamponade with air or gas (SF6, C3F8, etc.) is performed to attach the graft to the posterior stroma. Patients are required to maintain a supine position for several days postoperatively, and if graft detachment occurs, air reinjection (rebubbling) is performed. Postoperative steroid eye drops are continued for several months to over a year to prevent rejection, followed by low-dose maintenance therapy.
Cultured corneal endothelial cell injection therapy (regenerative medicine originating from Japan)
Kinoshita et al. developed a treatment in which cultured human corneal endothelial cells are injected into the anterior chamber together with the ROCK inhibitor Y-27632. It has been reported that corneal transparency was maintained after 5 years in 10 of 11 eyes with bullous keratopathy, with an average endothelial cell density of 1,257 cells/mm² 14). This treatment received manufacturing and marketing approval in Japan in 2022 after Phase II/III clinical trials, and is internationally recognized as regenerative medicine to compensate for donor corneal shortage 1,14).
The procedure of this therapy involves isolating and culturing endothelial cells from donor corneas, and injecting a cell suspension containing the ROCK inhibitor Y-27632 into the anterior chamber. After injection, the patient maintains a prone position (face down) for several hours to allow the cells to settle and adhere to the corneal endothelial surface by gravity. Compared to conventional corneal endothelial transplantation, this method requires smaller incisions and allows treatment of multiple cases from one donor cornea, which is also significant for effective use of donor corneas.
Treatment strategy is determined by comprehensively assessing the degree of edema progression, endothelial cell density, visual requirements, comorbidities, general condition, and patient preference. In mild or early cases, conservative treatment or ROCK inhibitor eye drops are used for observation; in moderate to advanced cases, endothelial transplantation is considered. In advanced cases with stromal opacity or vascular invasion, full-thickness corneal transplantation is selected. Even in cases indicated for surgery, if pain is the main complaint and visual prognosis is poor, symptomatic treatment with amniotic membrane transplantation or therapeutic PTK is useful.
QCan corneal transplantation be avoided with ROCK inhibitor eye drops?
A
In mild to moderate bullous keratopathy, ROCK inhibitor (ripasudil) eye drops have been reported to improve corneal edema and delay or avoid corneal transplantation in some cases. However, the effect is limited in advanced cases with severely reduced endothelial cells. Currently, ROCK inhibitor eye drops are not yet established as standard treatment, and the mainstay of curative treatment is corneal endothelial transplantation. Please consult your doctor to choose the appropriate treatment for your condition.
QCan cultured corneal endothelial cell injection therapy be received in Japan?
A
Yes, cultured corneal endothelial cell injection therapy received manufacturing and marketing approval in Japan in 2022. However, the number of facilities that can perform it is limited, and there are specific indications and eligibility criteria. It is not indicated for all patients with bullous keratopathy, and the decision should be made in consultation with your doctor. Amid the severe shortage of corneal donors, this Japanese regenerative medicine is expected to develop further.
The cornea maintains transparency by keeping a water content of about 78% (deturgescence). This relative dehydration is maintained by the balance of the following five factors.
Stromal swelling pressure (SP): approximately 50 mmHg. Glycosaminoglycans in the corneal stroma cause tissue expansion through anion repulsion, drawing fluid inward.
Epithelial barrier function: Tight junctions of the epithelium provide about twice the resistance to water inflow compared to the corneal endothelium.
Endothelial pump function: Active transport pumps fluid from the corneal stroma into the aqueous humor.
Tear evaporation: Osmotic withdrawal of water from the corneal surface.
Intraocular pressure (IOP): When IOP exceeds stromal swelling pressure, forward movement of fluid occurs.
Corneal endothelial fluid regulation is explained by Maurice’s pump-leak mechanism. Endothelial cells drive net ion flux from the corneal stroma to the anterior chamber via primary and secondary active transport mechanisms, creating an osmotic gradient. This pump function mainly depends on HCO₃⁻ and Cl⁻, with Na⁺/K⁺-ATPase playing a central role11).
In a healthy eye, the imbibition pressure IP is expressed as IP = IOP − SP, and is normally a negative pressure of about −35 to −45 mmHg. In endothelial dysfunction, stromal water increases and SP decreases; as it progresses, SP falls below IOP and IP becomes positive. Under positive pressure, water is pumped from the stroma to the epithelial side, forming epithelial edema and bullae. On the other hand, with high intraocular pressure (over about 50 mmHg), even if the endothelium is healthy, aqueous humor can be pushed into the epithelial layer causing epithelial edema, but in this case SP does not change and stromal edema does not occur.
Vicious cycle of Fuchs endothelial corneal dystrophy
According to Tone et al., in the early stages of Fuchs endothelial corneal dystrophy, a compensatory increase in Na⁺/K⁺-ATPase density is observed, but it gradually decreases as the disease progresses11). Real-time PCR detects significant downregulation of Na⁺/K⁺-ATPase density in advanced cases, along with downregulation of MCT1 and MCT4, confirming the failure of endothelial pump function. Increased corneal endothelial permeability (barrier dysfunction) has also been shown to precede pump dysfunction11).
Mechanisms of endothelial damage due to cataract surgery
Endothelial cell loss after cataract surgery occurs through multiple mechanisms. Mechanical and physical damage from intraoperative instruments or IOL contact and ultrasonic energy are the main causes; iris injury increases inflammatory cytokine levels in the anterior chamber, accelerating long-term endothelial loss1,2).
When corneal edema occurs in the presence of an IOL, it is defined as PBK even if corneal endothelial guttae are present. Unlike Fuchs endothelial corneal dystrophy, in PBK corneal edema tends to start peripherally and progress centrally.
When corneal endothelial cell density falls below approximately 2,000 cells/mm², permeability gradually increases, but deturgescence is maintained by compensatory pump mechanisms until around 500–400 cells/mm². Below this threshold, progression to bullous keratopathy is likely. However, the threshold varies among individuals; whether edema occurs at the same cell density depends on individual endothelial function.
Endothelial cell wound healing and compensatory mechanisms
Corneal endothelial cells do not undergo cell division in the anterior chamber environment. When a defect occurs, it is covered by enlargement and migration of surrounding cells. During this repair process, cell area increases, and pleomorphism and polymegethism become prominent. Specular microscopy quantifies these changes as an increase in the coefficient of variation (CV) and a decrease in the percentage of hexagonal cells. While cell density is high, pump function is maintained, but once the compensatory limit is reached, edema rapidly develops. Endothelial dysfunction may precede density decline, so the absolute density value alone cannot fully predict the onset of bullous keratopathy.
Chronic endothelial cell loss after cataract surgery and other intraocular procedures involves inflammatory cytokines in the anterior chamber (TNF-α, IL-1, IL-6). These cytokines induce apoptosis of endothelial cells, reducing both barrier and pump functions. Prolonged postoperative inflammation is an important risk factor for PBK1).
EndoArt (EyeYon Medical) is a dome-shaped artificial endothelial layer with a diameter of 6.0 mm and thickness of 50 μm, conforming to the curvature of the posterior corneal surface. Made of hydrophilic acrylic material, it is inserted into the anterior chamber using a technique similar to DMEK. Since it is non-biological, no immunosuppressive therapy is required, and it can be stored long-term. Auffarth et al. reported transplanting EndoArt in two cases of chronic corneal edema, with corneal thickness decreasing from 730 to 526 μm in case 1 and from 761 to 457 μm in case 2, remaining stable at 17 months12). It has received FDA Breakthrough Therapy Designation and is expected to be applied in complex eyes (aniridia, post-vitrectomy, tube-shunt eyes).
DSO is a surgical procedure that removes only the central Descemet membrane, allowing healthy peripheral endothelial cells to migrate and regenerate toward the center, thereby resolving corneal edema. Early-stage Fuchs endothelial corneal dystrophy was the main indication, but in recent years, its application to localized corneal edema such as that caused by MIGS tube contact has also been reported. Khan and Lin reported a case of corneal edema associated with Descemet membrane detachment after discontinuation of a MIGS device, in which DSO was performed; edema resolved after 6 weeks with eccentric descemetorrhexis, and central corneal endothelial cell density recovered from undetectable to 975 cells/mm² 13). The use of ROCK inhibitor eye drops (ripasudil, netarsudil) as an adjunctive therapy is also being considered.
For Fuchs endothelial corneal dystrophy, antisense oligonucleotides targeting the CTG repeat expansion in the TCF4 gene and molecular therapies targeting oxidative stress pathways are in the basic research stage. Abnormalities in oxidative stress pathways (decreased Nrf2/NQO1 signaling, mitochondrial dysfunction) have been shown to be involved in cell death, and the application of mitochondrial protective agents and antioxidants is being investigated.
Cell-Based Products and Advances in Regenerative Medicine
In addition to the cultured corneal endothelial cell injection therapy originating from Japan, research using iPS cells and stem cell-derived corneal endothelial cells is progressing in other countries. This approach has the potential to treat many eyes from a single donor cornea, and is expected as a solution to the global shortage of donor corneas 1,14). Furthermore, clinical trials are underway to evaluate the long-term efficacy and safety of ROCK inhibitors, quantitative assessment of endothelial cell migration, and optimal concentration and duration of administration.
For predicting the progression of bullous keratopathy and evaluating treatment response, research is being conducted on changes in central corneal thickness over time, endothelial cell density, detection of epithelial edema and microcysts using anterior segment OCT, and cytokine concentrations in tears. Improved accuracy of preoperative assessment is expected to enable early determination of the optimal treatment strategy (continuation of conservative treatment, ROCK inhibitor eye drops, endothelial transplantation, PK) for individual patients.
Bullous keratopathy often progresses bilaterally, and its impact on daily visual function is substantial. Morning vision loss interferes with housework and commuting, and as it progresses, reading, driving, and fine tasks become difficult. In recent years, efforts to evaluate patient-reported outcome measures (PROMs) related to visual function before and after surgery have advanced, and objective assessment of improvement in vision-related QOL is being used as an indicator for treatment selection 8). QOL assessments using the Visual Function Questionnaire-14 and NEI VFQ-25 before and after endothelial transplantation have shown a trend toward greater improvement in the DMEK group 8).
Treatment for bullous keratopathy is diversifying from full-thickness or endothelial transplantation using donor corneas to selective cell therapy, drug therapy, and artificial endothelial devices. The cultured corneal endothelial cell injection therapy developed in Japan is a pioneer in this field and is attracting attention as a solution to the global shortage of donor corneas. With the expansion of the application range of ROCK inhibitor eye drops, the clinical adoption of EndoArt, the expansion of indications for DSO, and the practical application of gene therapy, treatment options are expected to broaden further over the next decade. The goal is to reduce the need for corneal transplantation and greatly improve patients’ visual function and quality of life through early diagnosis and establishment of stepwise treatment strategies.
Jukić A, Pavan J, Đapic Ivančić B, Kalauz M, Kasalica Žužul R, Jukić T. RhoKinase (ROCK) Inhibition as a Therapeutic Strategy for Pseudophakic Bullous Keratopathy: A Comprehensive Review. Journal of clinical medicine. 2025;14(17). doi:10.3390/jcm14176093. PMID:40943853; PMCID:PMC12429473.
European Society of Cataract and Refractive Surgeons. ESCRS Clinical Guidelines for Cataract Surgery. 2024.
Singhal A, Kaushik J, Singh A, Shetty R. Descemet Stripping Endothelial Keratoplasty in Microcornea for Pseudophakic Bullous Keratopathy With Anterior Chamber Intraocular Lens. Cureus. 2021;13(11):e19262. doi:10.7759/cureus.19262. PMID:34900458; PMCID:PMC8648131.
Matthaei M, Hribek A, Clahsen T, Bachmann B, Cursiefen C, Jun AS. Fuchs Endothelial Corneal Dystrophy: Clinical, Genetic, Pathophysiologic, and Therapeutic Aspects. Annual review of vision science. 2019;5:151-175. doi:10.1146/annurev-vision-091718-014852. PMID:31525145.
Vandevenne MMS, Berendschot TTJM, Visser N, Dickman MM, Nuijts RMMA. Late-onset corneal edema after customized crosslinking for progressive keratoconus. American journal of ophthalmology case reports. 2024;35:102090. doi:10.1016/j.ajoc.2024.102090. PMID:38983453; PMCID:PMC11231532.
Chu MJ, Song M, Palmares T, Song A, Song J. Rhopressa-induced corneal edema: a case report. J Med Case Rep. 2021;15:182. doi:10.1186/s13256-021-02665-0.
Arici C, Mergen B, Kılıçarslan O, Ağaçhan A, Tülü Aygün B, Özdamar A. Diffuse corneal edema after uneventful pterygium surgery: toxic anterior segment syndrome or toxic keratopathy? Turk J Ophthalmol. 2022;52:69-71.
Farid M, Rhee MK, Akpek EK, Amescua G, Garcia-Ferrer FJ, Lin A, et al. Corneal Edema and Opacification Preferred Practice Pattern®. Ophthalmology. 2019;126(1):P216-P285. doi:10.1016/j.ophtha.2018.10.022. PMID:30366795.
Erdinest N, Shemesh N, Weill Y, Morad S, Nitzan I, Smadja D, et al. Managing pseudophakic bullous keratopathy with a topical rho kinase inhibitor: a case series. Journal of medical case reports. 2025;19(1):214. doi:10.1186/s13256-025-05263-6. PMID:40340708; PMCID:PMC12060286.
Tone SO, Kocaba V, Böhm M, Wylegala A, White TL, Jurkunas UV. Fuchs endothelial corneal dystrophy: the vicious cycle of Fuchs pathogenesis. Prog Retin Eye Res. 2021;80:100863. doi:10.1016/j.preteyeres.2020.100863. PMID:32438095; PMCID:PMC7648733.
Auffarth GU, Son HS, Koch M, Weindler J, Merz P, Daphna O, et al. Implantation of an Artificial Endothelial Layer for Treatment of Chronic Corneal Edema. Cornea. 2021;40(12):1633-1638. doi:10.1097/ICO.0000000000002806. PMID:34294634; PMCID:PMC8963521.
Khan NC, Lin CC. Descemet stripping only for Descemet’s membrane detachment and sectoral corneal edema. American journal of ophthalmology case reports. 2023;29:101784. doi:10.1016/j.ajoc.2022.101784. PMID:36619161; PMCID:PMC9811206.
Kinoshita S, Koizumi N, Ueno M, Okumura N, Imai K, Tanaka H, et al. Injection of Cultured Cells with a ROCK Inhibitor for Bullous Keratopathy. The New England journal of medicine. 2018;378(11):995-1003. doi:10.1056/NEJMoa1712770. PMID:29539291.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.