Epithelial downgrowth (also called epithelial ingrowth) is a complication in which non-keratinized stratified squamous epithelial cells from the conjunctiva or cornea enter the eye through an incompletely closed wound after penetrating ocular trauma or anterior segment surgery and proliferate on various intraocular tissues. The epithelium grows in sheets, spreading over the cornea, iris, trabecular meshwork, ciliary body, lens or intraocular lens, vitreous, and retina.
Glaucoma due to epithelial downgrowth is primarily caused by coverage and obstruction of the trabecular meshwork by proliferating epithelium, with inflammatory peripheral anterior synechiae and pupillary block also contributing. According to the EGS guidelines, treatment includes intraocular pressure-lowering medications, excision/destruction of invasive tissue, filtration surgery with antimetabolites (limited success), drainage devices, and cyclodestructive procedures1).
Most cases develop within one year of the causative event, but the range is from 3 months to 10 years postoperatively. Although the incidence has decreased significantly due to advances in surgical techniques, it is important to recognize this clinical entity because it is highly invasive and threatens visual function.
Membranous proliferation: appears as a translucent cystic or membranous growth with scalloped edges on the posterior corneal surface or anterior iris surface at the surgical incision site. The membrane extends from the wound and rarely extends beyond half of the cornea
Pupillary distortion: due to traction by the epithelial membrane
Corneal microcystic edema: appears in the affected area of the cornea
Intraocular pressure abnormality: may present with hypotony if a fistula is present; as trabecular meshwork obstruction progresses, elevated intraocular pressure and glaucoma may develop
QHow is epithelial ingrowth detected?
A
Typically, it is identified on slit-lamp examination as a translucent membrane with scalloped edges extending from the surgical wound. If the diagnosis is uncertain, a test using argon laser photocoagulation of the membrane on the iris is useful. If the membrane is present, the irradiated area becomes pale or white; in normal iris, dark coagulation spots appear. Alternatively, aqueous humor can be aspirated for cytology to check for free epithelial cells. Gonioscopy may reveal an epithelial sheet in the angle, but sensitivity is low, and many cases show normal findings.
Iris incarceration into the surgical wound: Iris incarceration into the wound promotes epithelial cell invasion
Vitreous prolapse: Vitreous prolapse into the wound is also a risk factor for epithelial ingrowth
Transplantation of epithelial cells by instruments: Surgical instruments carry corneal epithelial cells into the eye
Leakage from suture tracks: Microleaks provide a pathway for epithelial cells
Risk remains even with modern surgical techniques. Cases have been reported with clear corneal incision cataract surgery, glaucoma drainage device implantation, DSAEK, and LASIK.
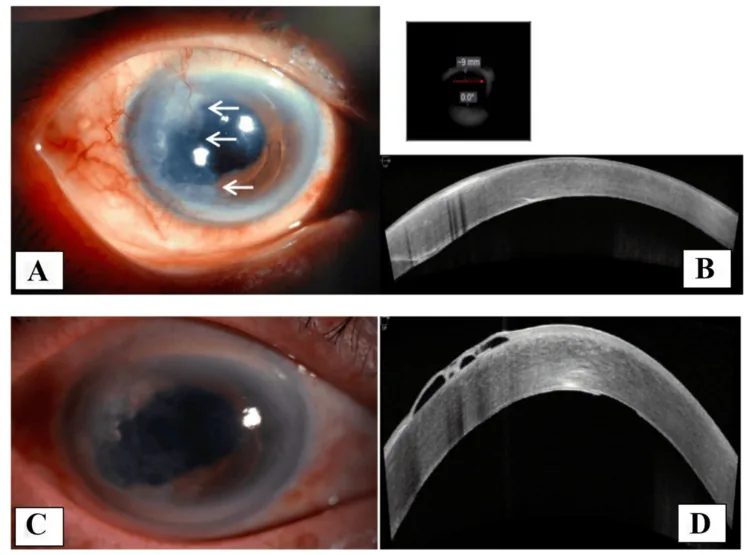
Cureus. 2025;17(4):e81948. Figure 3. PMCID: PMC12064144. License: CC BY.
A and C are anterior segment photographs showing membranous lesions on the posterior corneal surface, and B and D are corresponding AS-OCT images. They help visualize how epithelial downgrowth spreads into the anterior chamber.
Slit-lamp microscopy: Identify a semitransparent membrane on the posterior corneal surface or anterior iris surface, scalloped edges, and corneal microcystic edema.
Argon laser photocoagulation test: Spot irradiation is applied to the area covering the iris; if a membrane is present, it becomes pale or white. In a normal iris, dark coagulation spots appear.
Anterior chamber aspiration and cytology: To check for the presence of free epithelial cells.
Gonioscopy: To evaluate epithelial sheets in the angle and peripheral anterior synechiae. However, sensitivity is low, and most cases of glaucoma due to epithelial ingrowth show normal findings.
Histopathological examination: Epithelial cells are confirmed in surgical specimens. Immunohistochemical staining (pancytokeratin positive) is useful2).
En-bloc excision: Wide en-bloc excision of all involved tissues combined with full-thickness keratoplasty. This is the established standard treatment.
Cryotherapy: Indicated when only the posterior cornea, angle, or ciliary body is involved. It inactivates the ingrown epithelium but may require subsequent corneal transplantation due to endothelial cell loss.
Intracameral methotrexate injection: An alternative treatment with 400 μg/0.1 mL administered once weekly has been reported2). It suppresses epithelial ingrowth through antiproliferative effects and is less invasive than surgical excision2).
In glaucoma associated with epithelial ingrowth, aqueous outflow is severely reduced, so medication alone is usually insufficient.
Glaucoma drainage device: The mainstay of treatment. It is recommended to leave a longer intraocular portion or insert the tube through the pars plana to minimize epithelial cell invasion.
Trabeculectomy: Even with antimetabolites, it usually fails due to sheet-like invasion of epithelial cells.
QHow is glaucoma due to epithelial ingrowth treated?
A
Glaucoma drainage devices (tube shunt surgery) are the mainstay of treatment. Because aqueous outflow is significantly reduced, medication alone is usually insufficient. Trabeculectomy is not recommended as it often fails due to sheet-like invasion of epithelial cells. Cyclodestructive procedures are also used as additional intraocular pressure-lowering measures. For epithelial ingrowth itself, in addition to en bloc excision and cryotherapy, intracameral methotrexate injection has been reported as a minimally invasive alternative treatment.
Glaucoma due to epithelial ingrowth is multifactorial.
Direct coverage of trabecular meshwork: Proliferating epithelial sheets cover the trabecular meshwork, physically blocking aqueous outflow.
Mucin clogging: Mucin secreted by ectopic conjunctival goblet cells obstructs the trabecular meshwork.
Inflammatory changes: Epithelial proliferation and inflammation promote peripheral anterior synechiae formation, trabeculitis, and trabecular necrosis, further impairing aqueous outflow.
Pupillary block: Pupillary block can occur when adhesions form between the vitreous and the iris.
Steroid-induced intraocular pressure elevation: Steroid eye drops for epithelial ingrowth can lead to further intraocular pressure elevation.
According to the EGS guidelines, epithelial or fibrous ingrowth after anterior segment surgery or penetrating trauma can cause inflammatory membrane formation and lead to secondary glaucoma1).
QWhy does epithelial ingrowth cause glaucoma?
A
Multiple mechanisms are involved. The most primary mechanism is that the proliferating epithelial sheet directly covers the trabecular meshwork and blocks aqueous humor outflow. In addition, clogging of the trabecular meshwork due to mucin secretion from ectopic conjunctival goblet cells, peripheral anterior synechiae formation and trabecular necrosis due to inflammation, and pupillary block due to vitreous-iris adhesions also contribute. Steroid eye drops used for treatment may also cause further intraocular pressure elevation. As severe aqueous outflow obstruction results from these multifactorial causes, intraocular pressure control is often difficult with medication alone, and drainage devices are required.
Salari et al. reported weekly intracameral injections of methotrexate (MTX) 400 μg/0.1 mL for epithelial ingrowth occurring after Ahmed valve implantation2). After an initial 7 injections and 4 additional injections due to regrowth one month later (total 11 injections), the epithelial ingrowth disappeared, and no recurrence was observed during the 11-month follow-up period2). The antiproliferative effect of MTX is thought to contribute to the suppression of epithelial ingrowth2).
Although MTX has demonstrated safety and efficacy for intraocular administration in vitreoretinal lymphoma, further evidence is needed regarding the safety of intracameral administration2). Potential neuroretinal toxicity has been noted, and establishment of a dose-response curve is required2). The greatest advantage is that it is less invasive compared to surgical excision.
Prevention through Advances in Surgical Techniques
Advances in cataract surgery techniques (smaller and more precise wound creation) have significantly reduced the incidence of epithelial ingrowth. However, sporadic cases have been reported even with modern procedures such as clear corneal incision, glaucoma drainage device implantation, DSAEK, and LASIK.
Prevention remains paramount, and continued improvement in surgical techniques is expected to further reduce the incidence.
European Glaucoma Society. European Glaucoma Society Terminology and Guidelines for Glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. PMID:41026937. doi:10.1136/bjophthalmol-2025-egsguidelines.
2. Salari F, Fakhraie G, Asadi Amoli F, Zarei-Ghanavati M. Intracameral Injection of Methotrexate for Treatment of Epithelial Ingrowth. Journal of current ophthalmology. 2022;34(1):115-117. doi:10.4103/JOCO.JOCO_159_21. PMID:35620380; PMCID:PMC9128425.
Moshirfar M, Hall M, Ronquillo Y. Epithelial Downgrowth. . 2026. PMID: 32644422.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.