The stem cells of the corneal epithelium reside in the limbus, the border between the cornea and conjunctiva. The palisades of Vogt (POV) in the limbus function as a stem cell niche (microenvironment) and maintain corneal epithelial homeostasis.
When these limbal stem cells are extensively damaged, limbal stem cell deficiency (LSCD) occurs. In LSCD, corneal epithelial regeneration becomes impossible, and conjunctival epithelium invades the corneal surface (conjunctivalization) 4). This leads to corneal opacity, superficial neovascularization, and visual impairment.
Conventional corneal transplantation is ineffective for LSCD because the graft surface becomes conjunctivalized again, leading to failure 3). Therefore, ocular surface reconstruction is necessary to replenish normal corneal epithelial stem cells and stabilize the ocular surface.
The goal of reconstruction is not visual recovery but stabilization of the ocular surface. If corneal stromal opacity remains, full-thickness penetrating keratoplasty (PKP) or deep anterior lamellar keratoplasty (DALK) is performed in two stages after ocular surface stabilization.
QWhich patients are indicated for ocular surface reconstruction?
A
Patients with extensive damage to the limbal stem cells and invasion of conjunctival epithelium onto the cornea are candidates. Common causes include chemical burns, Stevens-Johnson syndrome, ocular cicatricial pemphigoid, and aniridia. In mild cases where conjunctival invasion is limited to the periphery, observation is initially performed.
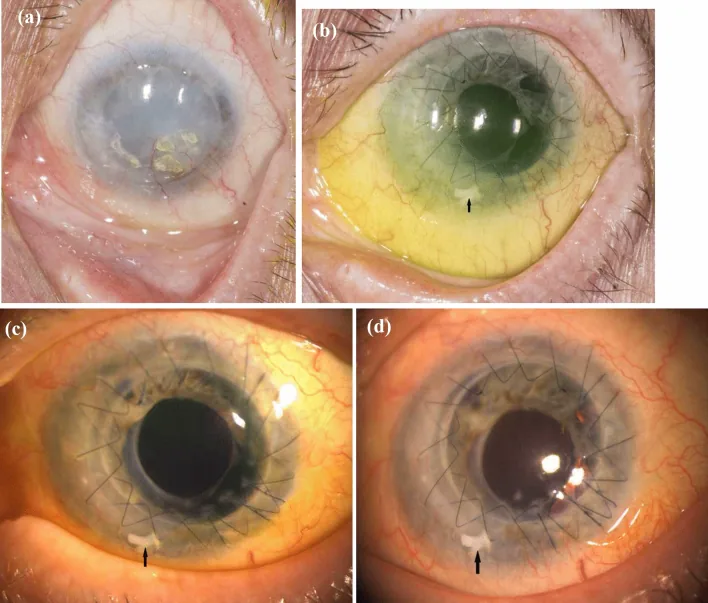
Anja Viestenz, Christiane Kesper, Thomas Hammer, Joana Heinzelmann, et al. ALT (allogeneic limbal transplantation): a new surgical technique for limbal stem cell deficiency 2022 Aug 19 Int Ophthalmol. 2022 Aug 19; 42(12):3749-3762 Figure 3. PMCID: PMC9617846. License: CC BY.
a shows preoperative diffuse corneal opacity and irregular surface. b to d show postoperative improvement in corneal clarity, with visible graft and sutures near the limbus.
The causes of LSCD are diverse, but chemical burns are the most common. In a systematic review of autologous limbal transplantation, 88% of the treated eyes had chemical burns 3).
The main causes are listed below.
Chemical burns (alkali/acid): Most common cause. Alkali penetrates deeply due to pH elevation and extensively destroys limbal stem cells4). Often occurs in the workplace and is more common in low-income populations 4).
Thermal burns: Thermal coagulation of the cornea from hot metal, flames, etc.
This is the most basic diagnostic method. It evaluates the loss of the palisades of Vogt (POV), the extent of conjunctivalization, and the degree of superficial neovascularization. Normally, POV are easily observed in the superior and inferior limbus, but may be difficult to observe in individuals aged 10 years or younger and 70 years or older.
Cells from the corneal surface are collected and immunostained. Loss of corneal epithelial markers cytokeratin 3 (CK3)/CK12 and expression of conjunctival epithelial markers CK13/MUC5AC are useful for definitive diagnosis of LSCD1).
Non-invasively evaluates changes in corneal epithelial thickness and structure. Conjunctivalized areas show a different reflection pattern from normal corneal epithelium.
Allows observation of POV structures and basal cell morphology at the cellular level. It is also useful for distinguishing corneal epithelium from conjunctival epithelium, but the equipment is only available in limited facilities.
The choice of treatment differs greatly depending on whether the disease is unilateral or bilateral. In unilateral LSCD, autologous tissue can be harvested from the healthy eye’s limbus, but in bilateral cases, autologous limbal tissue is not available, so alternative cell sources such as oral mucosal epithelium are used.
Analysis of CLAu 22 case series (1023 eyes), SLET 4 studies (253 eyes), CLET 8 studies (581 eyes). 88% of CLAu subjects and over 90% of CLET/SLET subjects had chemical burns. SLET and CLAu had significantly higher anatomical success rates compared to CLET. 3)
Mazumdar et al. reported a case of unilateral LSCD due to alkali injury treated with simultaneous SLET and conjunctival autograft in a single stage 2).
A 24-year-old male with stage III LSCD after alkali injury. Corneal epithelialization was completed 24 days postoperatively, and best corrected visual acuity (BCVA) of 6/12p was achieved at 24 months of follow-up. The advantage of simultaneous conjunctival defect repair and limbal reconstruction in a single-stage surgery was demonstrated. 2)
If corneal stromal opacity persists after ocular surface reconstruction, full-thickness corneal transplantation or DALK is added. DALK is preferable to avoid endothelial rejection. Long-term administration of immunosuppressive drugs (cyclosporine, tacrolimus) may be necessary.
QWhy does treatment differ between unilateral and bilateral cases?
A
In unilateral cases, corneal epithelial stem cells can be harvested from the limbus of the healthy contralateral eye. In bilateral cases, both eyes have limbal damage, so corneal epithelial stem cells cannot be harvested. Therefore, cultured oral mucosal epithelial transplantation (COMET) using alternative cell sources such as oral mucosal epithelium is selected.
QHow long after surgery does vision recover?
A
The main goal of ocular surface reconstruction is stabilization of the ocular surface, and it does not guarantee direct visual recovery. If the corneal stroma is opaque, a two-stage treatment involving corneal transplantation after reconstruction is necessary. Visual improvement may take several months to over a year.
Corneal epithelial stem cells reside within the palisades of Vogt (POV) in the basal layer of the limbus. The POV consists of papillary projections of the stroma, richly supplied with blood vessels and nerves. This microenvironment (niche) regulates the self-renewal and differentiation of stem cells.
Stem cells undergo asymmetric division to self-renew while producing transit amplifying cells (TACs). TACs migrate toward the central cornea, dividing and differentiating, eventually becoming corneal epithelial cells that shed from the surface.
When limbal stem cells are damaged, the following pathological processes occur in a cascade.
Cessation of corneal epithelial replenishment
Invasion of conjunctival epithelium onto the corneal surface (conjunctivalization)
Appearance of goblet cells on the cornea (MUC5AC positive)
Superficial neovascularization and chronic inflammation
Corneal stromal scarring
The conjunctivalized corneal surface has reduced barrier function, leading to recurrent persistent epithelial defects. Persistent inflammation may also cause stromal melting or perforation.
Techniques for preparing cultured epithelial sheets
In COMET (cultured oral mucosal epithelial transplantation), the temperature-responsive culture dish is a core technology 1). The poly(N-isopropylacrylamide) coating on the dish surface is hydrophobic at 37°C and becomes hydrophilic when the temperature is lowered. This allows the cell sheet to be detached from the dish without enzymatic treatment, enabling transplantation while maintaining cell-cell adhesion and matrix 1).
Post-transplant evaluation using stem cell markers
In Japan, in June 2021, the world’s first COMET product Ocural® was covered by insurance 1). Ocural® is indicated for bilateral LSCD without symblepharon. For cases with symblepharon, Sakracy® is selected 1).
Toshida et al. reported the initial results of two cases treated with Ocural®. Case 1 was a 79-year-old male (bilateral stage III LSCD), and case 2 also had bilateral LSCD; engraftment was confirmed in both. Post-transplantation sheets showed expression of p63, p75NTR, and Ki-67, indicating maintenance of stem cell characteristics and proliferative capacity. 1)
For unilateral LSCD, Nepic® (cultured autologous limbal epithelial cell sheet) can be used 1).
In Europe, Holoclar® was the first cultured autologous limbal epithelial transplant to be approved as a medicinal product in the EU 1). It is a pioneer in regenerative medicine for LSCD treatment and takes a different approach (limbal epithelium-derived vs. oral mucosal epithelium-derived) from Japan’s Ocural®.
Mazumdar et al. reported that combining SLET and conjunctival autograft (CAG) in a single stage simultaneously achieved conjunctival defect repair and limbal reconstruction. Complete epithelialization occurred by postoperative day 24, and BCVA improved to 6/12p at 24 months. 2)
In conventional SLET, the conjunctival defect is left as exposed sclera or covered with amniotic membrane, but concurrent CAG may provide early conjunctival coverage and a stable ocular surface 2).
Comparison of Outcomes Between Surgical Techniques
In a systematic review by Shanbhag et al. (1857 eyes), overall anatomical success rate for autologous limbal transplantation was 69%, and functional success rate was 61%. By technique, SLET and CLAu showed significantly better outcomes than CLET. However, there were significant differences in study quality and sample size between groups, requiring caution in interpretation. 3)
Future accumulation of randomized controlled trials and long-term outcomes is needed. Next-generation cell therapies, such as corneal epithelial cell sheets derived from iPS cells, are also under research.
Long-Term Challenges of Cultured Oral Mucosal Epithelium
Cultured autologous oral mucosal epithelial cell sheets (CAOMECS) were reported in 2004 and have confirmed efficacy as an autograft for bilateral LSCD. However, long-term observation has shown re-opacification due to vascular invasion from the peripheral cornea in some cases. Differences in properties between corneal epithelium and oral mucosal epithelium are suggested as the cause, and the use of corneal epithelial cells themselves is considered more desirable for curative treatment.
Research on corneal regeneration using cell sources other than limbal stem cells is progressing.
Mesenchymal stem cells (MSCs): There is a report of reconstructing the rat corneal surface by transplanting bone marrow-derived MSCs onto human amniotic membrane. It has been suggested that suppression of inflammation and angiogenesis, rather than epithelial differentiation, may be involved in the therapeutic effect. Adipose-derived MSCs have been confirmed to differentiate into functional corneal stromal cells after intrastromal injection.
Dental pulp stem cells: Isolated from deciduous teeth, they express limbal stem cell markers. Ocular surface reconstruction has been demonstrated in a rabbit model, but efficacy in humans has not been confirmed.
Hair follicle stem cells: Reprogramming to a corneal epithelial phenotype using conditioned medium derived from corneal and limbal stroma has been demonstrated in vitro.
The presence of progenitor cells has also been shown in the corneal stroma, and research is progressing on new treatments for corneal endothelium, such as for bullous keratopathy.
QIs cultured epithelial transplantation covered by insurance in Japan?
A
Yes, in 2021, the COMET product Ocural® was covered by insurance. However, it is limited to facilities with ophthalmologists who are members of the Japan Cornea Society and the Japan Corneal Transplantation Society and have completed the prescribed training. The indication is moderate to severe limbal stem cell deficiency.
Toshida H, Seki T, Kuroda M, et al. Early Clinical Outcomes of the First Commercialized Human Autologous Ex Vivo Cultivated Oral Mucosal Epithelial Cell Transplantation for Limbal Stem Cell Deficiency: Two Case Reports and Literature Review. Int J Mol Sci. 2023;24(10):8926. doi:10.3390/ijms24108926. PMID:37240280; PMCID:PMC10219018.
Mazumdar S, Trehan HS, Agarwal T, et al. Autologous simple limbal stem cell transplantation with conjunctival autograft in a case of unilateral limbal stem cell deficiency secondary to alkali injury. BMJ Case Rep. 2024;17:e261555.
Shanbhag SS, Nikpoor N, Rao Donthineni P, Singh V, Chodosh J, Basu S. Autologous limbal stem cell transplantation: a systematic review of clinical outcomes with different surgical techniques. The British journal of ophthalmology. 2020;104(2):247-253. doi:10.1136/bjophthalmol-2019-314081. PMID:31118185.