Chemical injury (alkali burn) is a condition in which the cornea and conjunctiva are damaged by alkaline chemicals entering the eye. It is one of the most urgent ophthalmic emergencies, and immediate response determines the prognosis.
The incidence of ocular chemical injury is estimated at 65–78 per 100,000 population 1). The mean age is 48 years, but there is a bimodal peak including those under 1 year of age 1). Alkali injuries are more common than acid injuries 1). Workplace injuries are the most frequent, and among occupational eye injuries, they are the second most common after metallic foreign bodies 1). Alkali injuries due to assault often reach Roper-Hall Grade IV severity, and ammonia-related assaults have been reported to result in the worst outcomes 1).
The main causative substances of alkaline materials are shown below. Note that even household products can cause severe eye injury.
Causative substance
Examples of products containing it
Characteristics
Sodium hydroxide
Mold remover, drain cleaner
Reaches anterior chamber within minutes
Ammonia
Hair dye, industrial cleaner
Penetrates cornea instantly
Potassium hydroxide
Industrial cleaner
High tissue penetration
Lime/cement
Construction materials (slaked lime, quicklime)
Common in occupational injuries
Quicklime (calcium oxide)
Desiccant, building materials
Accompanied by exothermic reaction
Compared to acidic substances, alkalis saponify lipids and cause cell lysis and necrosis. Since they do not form a barrier of coagulated proteins, they have high deep penetration and can reach the anterior chamber, causing iritis, cataract, and glaucoma. Therefore, alkali injuries tend to cause more severe damage overall than acid injuries.
QWhy are alkali injuries more severe than acid injuries?
A
Alkalis saponify cell membrane lipids via hydroxide ions, causing lysis and necrosis. While acids form a barrier of coagulated proteins that limits damage to the surface (except for strong acids and hydrofluoric acid), alkalis do not form such a barrier and penetrate deep into the cornea and anterior chamber within a short time. Ammonia penetrates the cornea instantly, and sodium hydroxide reaches the anterior chamber within minutes, causing iritis, traumatic cataract, and secondary glaucoma.
Eslani M, Baradaran-Rafii A, Movahedan A, Djalilian AR. The Ocular Surface Chemical Burns. J Ophthalmol. 2014;2014:196827. Figure 1. DOI: 10.1155/2014/196827. PMCID: PMC4106115. License: CC BY.
Anterior segment 8 days after alkali burn. A white ischemic area (avascular limbus) with loss of vascular network is clearly visible at the inferonasal limbus, and the surrounding conjunctiva shows injection and edema. This corresponds to limbal ischemia (bloodless limbus) discussed in the section “Main symptoms and clinical findings.”
In mild cases, conjunctival injection and partial corneal epithelial defects are observed. In severe cases, the entire cornea appears white and opaque, and with conjunctival necrosis, it may appear white and edematous without injection. This finding can appear mild at first glance, so caution is needed.
Evaluation of corneal epithelial defects with fluorescein staining is an essential examination. However, when the corneal and conjunctival epithelium is extensively damaged, the entire area may stain thinly and uniformly, making it appear as if there are no epithelial defects, so caution is needed to avoid underestimation.
Alkali-specific complications include iritis, traumatic cataract, and acute glaucoma due to anterior chamber penetration, which can occur from the acute phase. During the cicatricial phase, the following complications become problematic.
QWhy is there no hyperemia in severe alkali injury?
A
In severe alkali injury, extensive conjunctival necrosis occurs, and conjunctival vessels are also damaged. The necrotic tissue appears white and edematous, presenting a white appearance without hyperemia. This can easily lead to a misjudgment that “no hyperemia = mild case.” In reality, it indicates extensive ischemia including limbal vessels, suggesting a poor prognosis.
The degree of penetration of alkaline substances depends on the type of agent, pH, concentration, contact time, and area of injury.
Ammonia has particularly high tissue permeability, penetrating the corneal stroma instantly and reaching the anterior chamber. Sodium hydroxide (e.g., in mold removers) also reaches the anterior chamber within minutes, damaging the corneal endothelium, iris, and lens.
Risk factors include the following:
Occupational exposure: Construction work (cement, lime), cleaning work (strong alkaline cleaners), beauty industry (hair dye)
Household accidents: Misuse of mold removers, drain cleaners, hair dyes
Assault: Violent acts involving ammonia spray. These are often the most severe cases1)
Children: Misuse of desiccants (quicklime) or detergents. Peak incidence occurs under 1 year of age1)
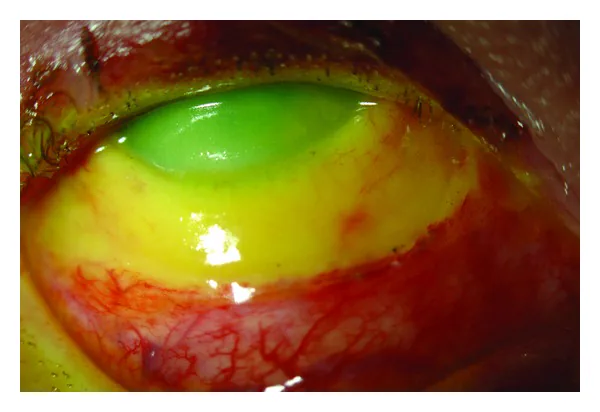
Eslani M, Baradaran-Rafii A, Movahedan A, Djalilian AR. The Ocular Surface Chemical Burns. J Ophthalmol. 2014;2014:196827. Figure 2. DOI: 10.1155/2014/196827. PMCID: PMC4106115. License: CC BY.
Roper-Hall Grade IV alkali burn. Fluorescein staining reveals epithelial loss over the entire cornea (green fluorescent area), with extensive severe conjunctival ischemia and necrosis (yellow-white necrotic tissue) extending more than 4 mm from the limbus. This corresponds to Roper-Hall Grade IV discussed in the “Diagnosis and Examination Methods” section.
The Kinoshita classification is a severity classification based on the extent of remaining POV (palisade of Vogt: corneal epithelial stem cell niche at the limbus), allowing prognosis estimation from slit-lamp findings at the initial examination.
Limbal conjunctival necrosis involving more than half the circumference, total corneal epithelial defect, complete loss of POV
Poor
The Roper-Hall classification is a 4-grade system based on the degree of corneal opacity and the extent of limbal ischemia 1). The Dua classification further subdivides Roper-Hall Grade IV into three grades (Dua grade IV: limbal involvement 50–75%, grade V: 75–100%, grade VI: 100%) 1). Early amniotic membrane transplantation is effective in Dua grades IV and V, but its benefit is limited in grade VI 1).
AS-OCTA (anterior segment optical coherence tomography angiography) is useful for evaluating limbal ischemia. Clinical assessment alone tends to underestimate the extent of limbal ischemia, and objective evaluation with AS-OCTA improves the accuracy of prognosis prediction 2).
QHow to differentiate between the Kinoshita classification and the Roper-Hall classification
A
The Kinoshita classification focuses on the presence or absence of residual POV (corneal epithelial stem cell niche) and directly reflects the potential for epithelial regeneration, making it superior for prognosis prediction. The distinction between Grade 3a and 3b (residual vs. complete loss of POV) greatly influences treatment strategy. The Roper-Hall classification is an international 4-grade system combining the degree of corneal opacity and the extent of limbal ischemia, while the Dua classification further subdivides Roper-Hall Grade IV into three severity grades to aid in determining surgical treatment indications 1).
The severity and healing time of alkali burns can be reduced by immediate copious irrigation. The time from injury to initial irrigation significantly affects visual prognosis.
Irrigation at the scene: Use a faucet directed upward or a hose, and continue for at least 20 minutes.
Eye irrigation at the ophthalmologist: After topical anesthesia, irrigate the conjunctival sac with 500–2,000 mL of normal saline or lactated Ringer’s solution. For severe alkali injuries, irrigate for 30 minutes or more.
Choice of irrigation solution: Tap water is hypotonic and increases water influx into the corneal stroma, so an isotonic solution (normal saline or lactated Ringer’s solution) is preferable.
Recheck pH: Recheck pH 20 minutes after irrigation, and re-irrigate if necessary.
Necrotic tissue removal and amniotic membrane transplantation (to reduce inflammation and promote epithelialization) are performed. Tenonplasty is a procedure that advances Tenon’s capsule to the limbus to restore vascular supply in cases of limbal and scleral ischemia, and is useful as an eye-preserving surgery in severe chemical trauma2). The postoperative re-epithelialization rate is high, but symblepharon is the most common complication2).
Subacute phase and cicatricial phase (Grade 3a):
If limbal function is preserved, the corneoconjunctival epithelium regenerates, sometimes resolving with residual pseudopterygium or corneal opacity. Amniotic membrane covering may be performed to promote early epithelialization.
Cicatricial phase (Grade 3b and 4):
In severe cases with complete loss of limbal epithelium, limbal function is lost, and conjunctival epithelium invades the cornea. Persistent corneal epithelial defects may lead to corneal melting and perforation. In the cicatricial phase, the following ocular surface reconstruction procedures are considered.
Keratoplasty for epithelialization (KEP): Performed for persistent corneal epithelial defects
Corneal limbal transplantation (auto/allograft): Replacement of limbal stem cells
Cultured epithelial cell sheet transplantation: Using autologous or allogeneic cultured epithelial cells
Corneal transplantation (lamellar or penetrating): In cases of perforation due to persistent epithelial defects
Chronic phase (persistent epithelial defect for more than 1 month after injury):
If corneal opacity remains in the cicatricial stage, superficial or full-thickness corneal transplantation is performed if the opacity is limited to the central area and some POV is preserved. If POV is completely lost and the corneal surface is covered by conjunctival tissue, corneal transplantation is performed after reconstructing the ocular surface with KEP, limbal transplantation, or amniotic membrane transplantation. To avoid endothelial rejection, DALK (deep anterior lamellar keratoplasty) may be selected in some cases.
For bilateral severe chemical trauma, a one-stage procedure using femtosecond laser-assisted large-diameter lamellar keratolimbal transplantation for simultaneous transplantation of limbal stem cells and corneal stroma has been reported, achieving good visual improvement3).
QHow long should eye irrigation be performed?
A
At the scene, it is desirable to continue for at least 20 minutes and as long as possible. For severe alkali injuries, irrigation should be continued for 30 minutes or more even after ophthalmological consultation. Tap water is readily available but hypotonic; therefore, isotonic solutions such as normal saline or lactated Ringer’s solution are recommended for irrigation in ophthalmology. Irrigation should take priority over ophthalmological evaluation, and whether sufficient irrigation has been performed before arrival significantly affects the prognosis.
Alkaline substances saponify the lipids of cell membranes via hydroxyl ions, causing cell lysis and necrosis. They dissolve proteins and reach the deep cornea, causing more severe damage than acids. Since they do not form a barrier of coagulated proteins, they penetrate deep into the corneal stroma and anterior chamber within a short time.
Alkali that penetrates the anterior chamber causes iritis, traumatic cataract, and acute glaucoma (severe intraocular pressure elevation in the acute phase). Ammonia is particularly permeable and penetrates the cornea instantly, while sodium hydroxide reaches the anterior chamber within minutes.
The degree of damage to corneal epithelial stem cells located in the palisades of Vogt (POV) of the limbus determines the prognosis.
Grade 1–3a (POV preserved): Even if the corneal epithelium is extensively lost, the limbal epithelium remains, so the corneal epithelium regenerates over time, and the prognosis is relatively good.
Grade 3b–4 (POV completely lost): Regeneration as transparent corneal epithelium becomes difficult. The less transparent conjunctiva covers the cornea with vascular invasion (conjunctivalization).
As conjunctivalization progresses, mucin deficiency due to goblet cell damage, tear film instability, symblepharon, and conjunctival sac shortening further worsen the ocular surface environment. Limbal ischemia increases the risk of limbal stem cell deficiency (LSCD), leading to corneal scarring and permanent visual impairment2).
Acute phase (injury to 7 days): Mainly corneal and conjunctival epithelial damage and acute inflammation
Early repair phase (8–21 days): Attempts at epithelial regeneration and prolonged inflammation
Late repair/scarring phase (day 22 onward): Scarring, conjunctivalization, stabilization or worsening of the ocular surface environment.
In difficult cases, ocular surface reconstruction is often challenging, and immediate irrigation after injury followed by appropriate treatment are key factors determining the prognosis of the ocular surface.
AS-OCTA objectively quantifies limbal ischemia in the acute phase of chemical injury, allowing more accurate assessment of ischemic areas that tend to be underestimated by clinical evaluation alone. It also correlates well with final visual prognosis, and integration into existing severity classification systems is anticipated 2).
Femtosecond laser-assisted large-diameter lamellar keratolimbal transplantation is a surgical technique that allows simultaneous transplantation of limbal stem cells and corneal stroma in a single stage for severe bilateral chemical trauma. Compared to conventional manual dissection, it enables uniform lamellar dissection, and good visual improvement has been reported3).
Femtosecond laser applications are limited in the number of cases, and further research is needed to establish long-term efficacy 3). Standardization of AS-OCTA and its incorporation into severity classification systems remain future challenges 2).
Chemical injuries of the eye. Ann Eye Sci. 2023;8:13.
Sharma S, Kate A, Donthineni PR, Basu S, Shanbhag SS. The role of Tenonplasty in the management of limbal and scleral ischemia due to acute ocular chemical burns. Indian journal of ophthalmology. 2022;70(9):3203-3212. doi:10.4103/ijo.IJO_3148_21. PMID:36018089; PMCID:PMC9675520.
Lin L, Xu Y, Ou Z, Zhuo K, Tian D, Chen J, et al. Femtosecond laser-assisted large-diameter lamellar corneal-limbal keratoplasty in ocular chemical burns. American journal of ophthalmology case reports. 2025;37:102246. doi:10.1016/j.ajoc.2024.102246. PMID:39839915; PMCID:PMC11745959.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.