Corneal epithelial abrasion refers to a condition where the entire corneal epithelium is lost. It is also called simple corneal erosion.
The corneal epithelium consists of 5 to 6 layers of stratified squamous epithelium and sits on the basement membrane. Under normal conditions, turnover occurs approximately every 7 days, protecting the eye from mechanical and chemical stimuli from the outside. When the entire epithelium is lost, the basement membrane is exposed, directly stimulating the corneal nerve endings, causing severe pain, tearing, and redness.
Traumatic corneal epithelial abrasion is one of the most common eye injuries in daily practice. Typical mechanisms include mechanical irritation from contact lenses, scratches from paper, fingernails, or leaf edges, and foreign body entry.
Clinically, it is broadly classified into two types based on the onset mechanism and healing course.
Simple corneal epithelial defect (simple corneal erosion): An acute epithelial defect due to a single cause such as trauma, with a tendency to heal spontaneously.
Persistent epithelial defect (PED): A full-thickness defect of the corneal epithelium that persists for more than one week due to various causes (internationally, many reports use a criterion of more than two weeks) [5]. Simple observation does not lead to healing, and investigation and treatment of the underlying disease are necessary.
QAre corneal epithelial abrasion and corneal erosion the same disease?
A
A condition in which the entire layer of the corneal epithelium is missing is called corneal epithelial defect (simple corneal erosion). It is almost synonymous with corneal erosion in the narrow sense. On the other hand, superficial punctate keratopathy (SPK) is a partial, punctate disorder of the epithelium and is distinguished from corneal epithelial defect, which involves full-thickness epithelial loss.
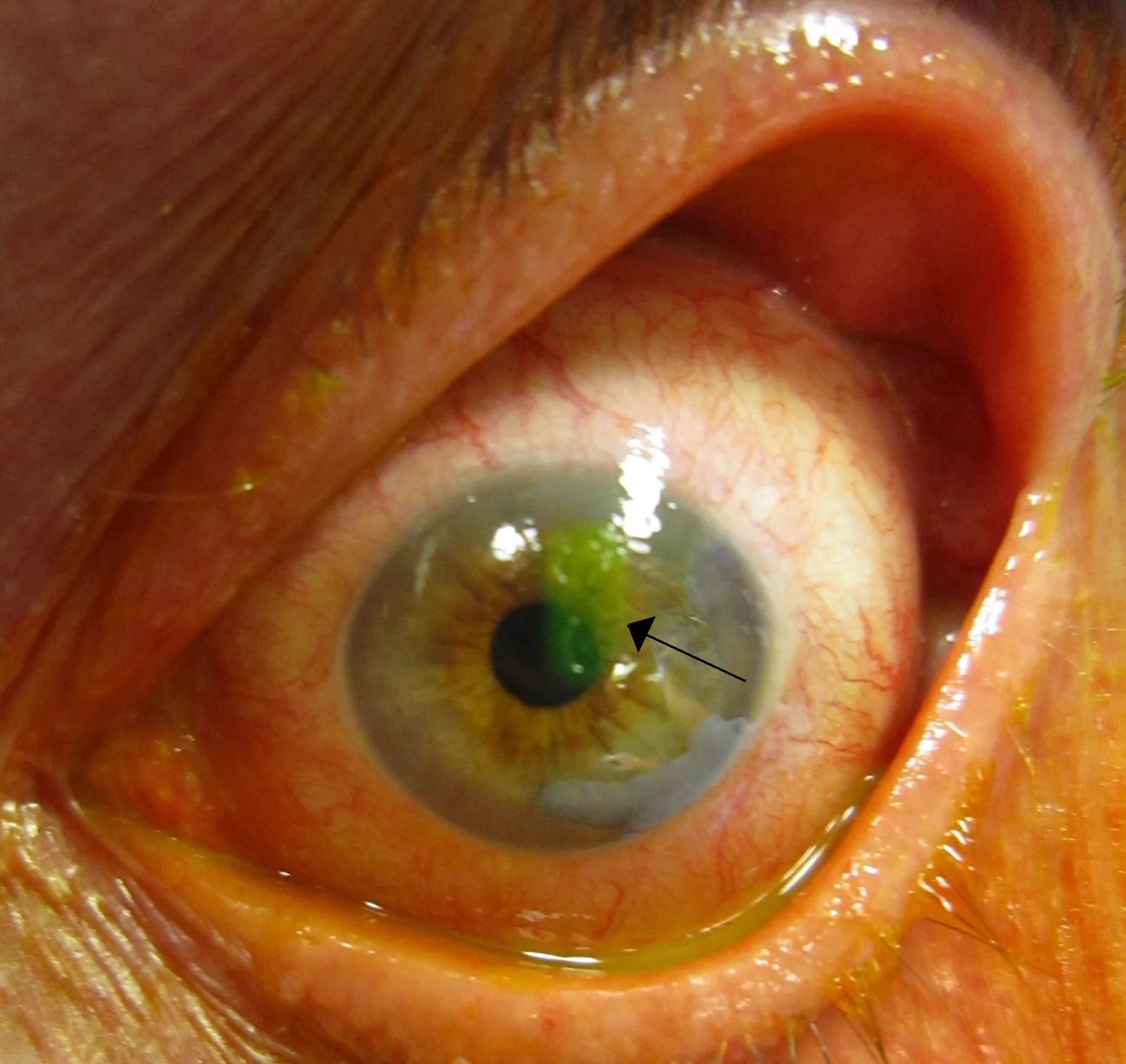
Clinical photograph of corneal epithelial defect showing positive fluorescein staining. This corresponds to the fluorescein-positive corneal epithelial defect finding discussed in the section “2. Main symptoms and clinical findings.”
Corneal epithelial defect often presents with pain, tearing, and redness. Pain is due to exposure of corneal nerve endings and may be accompanied by difficulty opening the eye. In patients with predisposing factors such as diabetes or those using steroid eye drops, special attention to infectious complications is necessary.
Pain may increase when systemic blood circulation is enhanced, such as during bathing or alcohol consumption. It is advisable to instruct patients to refrain from bathing and drinking alcohol on the day of injury.
By combining slit-lamp microscopy with fluorescein staining, an epithelial defect with clear margins is clearly observed. Fluorescein is taken up by the epithelial defect and fluoresces a bright yellow-green under cobalt blue light.
Clinical findings of simple corneal erosion
Subjective symptoms: Acute severe pain, tearing, redness
Fluorescein staining findings: Epithelial defect with clear margins, typically a single lesion with sharp borders
Course: Usually the epithelium regenerates in 2–3 days and heals without opacity
Clinical findings of persistent epithelial defect (PED)
Course: Does not heal within one week. Becomes refractory without treatment of the underlying disease
PED typically presents with a horizontally oval epithelial defect and a rolled-up edge at the defect margin. As the lesion progresses, it may be accompanied by ground-glass stromal opacity.
Beta-blocker eye drops, aminoglycosides, diclofenac sodium eye drops, frequent use of oxybuprocaine, steroid eye drops, antineoplastic agents
In neurotrophic keratopathy due to trigeminal nerve palsy, corneal sensation is reduced, so pain is mild and patients are often slow to notice. It frequently occurs after diabetes, herpes keratitis, or acoustic neuroma resection, and caution is needed to avoid overlooking it.
In limbal stem cell deficiency, depletion of limbal epithelial stem cells leads to loss of epithelial regenerative capacity, resulting in a particularly poor prognosis. It is associated with Stevens-Johnson syndrome, ocular cicatricial pemphigoid, GVHD, and chemical injury (alkali/acid), so a history of these diseases must always be confirmed through interview.
In drug-induced PED, frequent use of topical anesthetics (oxybuprocaine) is particularly important because it is directly toxic to the corneal epithelium. Frequent use for pain relief can lead to toxic keratopathy, so unnecessary prescriptions to patients must be absolutely avoided.
QWhy do contact lenses damage the cornea?
A
The main causes are mechanical friction from contact lens (CL) wear, impaired epithelial metabolism due to poor oxygen permeability, and foreign bodies trapped under the lens. Improper use (prolonged wear, insufficient cleaning, wearing dirty lenses) increases the risk. Regular lens replacement and proper care products are essential for prevention.
Fluorescein staining is essential for diagnosing corneal epithelial defects. Under a slit lamp with a cobalt blue filter, fluorescein staining shows the defect as a bright yellow-green fluorescence. In simple cases, it appears as a well-defined defect.
If the defect does not heal within one week, perform the following detailed examination for PED.
Corneal sensitivity measurement: If hypoesthesia is present, suspect neurotrophic keratopathy.
Assessment of tear secretion: Evaluation of tear volume using the Schirmer test.
Observation of POV (palisades of Vogt): Assess the status of limbal epithelial stem cells.
History of medications and surgeries: History of frequent use of beta-blockers, aminoglycosides, steroids, oxybuprocaine, and history of corneal transplantation or glaucoma surgery.
Antibiotic eye drops are used to prevent infection, and hyaluronic acid preparations are used to promote epithelial regeneration. If pain is severe, antibiotic eye ointment is used for relief and the eye is closed with an eye patch. If this is insufficient, oral analgesics are prescribed. The effectiveness of prophylactic antibiotics has been examined in a Cochrane review, but evidence is currently insufficient [1]. Additionally, it has been reported that indiscriminate use of pressure patching for pain relief increases the risk of complications and is not recommended [2].
An eye patch is used to close the eyelid when pain is severe. The patch blocks air stimulation to the corneal surface, effectively reducing pain.
Simple corneal epithelial defects usually heal within 2-3 days with epithelial regeneration, without leaving visual impairment or corneal opacity. Rarely, they may progress to recurrent corneal erosion, so follow-up is needed to check for recurrence after treatment.
In the treatment of PED, priority is given to treating the underlying disease. The treatment strategy is selected according to the cause.
Neurotrophic keratopathy: For diseases that can improve corneal sensation (e.g., better glycemic control in diabetes), intervention for the underlying disease is performed. Locally, protection of the ocular surface with therapeutic contact lenses and promotion of epithelial regeneration with autologous serum eye drops are considered effective.
Limbal stem cell deficiency: When limbal stem cells are depleted due to Stevens-Johnson syndrome, ocular cicatricial pemphigoid, GVHD, etc., cultured epithelial sheet transplantation or corneal limbal transplantation may be necessary. If stem cell damage is circumferential, the prognosis is poor, and long-term management at a specialized facility is required.
Drug-induced PED: Discontinuation of the causative drug is the most important intervention. Improvement can be expected by stopping beta-blocker eye drops, aminoglycosides, diclofenac sodium, and steroid eye drops.
QCan I get painkiller eye drops?
A
Prescribing topical anesthetics (e.g., oxybuprocaine) for pain relief is strictly prohibited as it causes toxic keratopathy. For pain, manage with oral analgesics such as loxoprofen Na 60 mg and eyelid closure with antibiotic ointment. Oral analgesics should be prescribed and taken according to the dosage.
QHow many days does it take for corneal epithelial detachment to heal?
A
In simple cases, the defect is usually covered within 2-3 days by epithelial migration and proliferation, and heals without opacity or visual impairment. If healing does not occur within one week, suspect persistent corneal epithelial defect (PED) and investigation of the cause is necessary.
The corneal epithelium consists of 5-6 layers of stratified squamous epithelium and is located on the basement membrane (above Bowman’s layer). Epithelial cells are supplied from limbal epithelial stem cells, differentiate and migrate from basal cells to wing cells to superficial squamous cells, and turn over approximately every 7 days. Basal cells are anchored by hemidesmosomes and basement membrane adhesion complexes; disruption of this adhesion predisposes to epithelial detachment.
When the full thickness of the corneal epithelium is lost due to trauma, the basement membrane is exposed. The basement membrane contains abundant corneal sensory nerve endings, and exposure allows direct action of physical stimuli and chemical mediators, causing severe pain.
In the normal healing process, basal cells at the wound margin migrate to the epithelial defect, then proliferate to cover the defect. This migration and proliferation process usually covers the defect with epithelium within 2 to 3 days. Hyaluronic acid preparations promote epithelial cell migration and adhesion, accelerating healing.
In some cases, even after healing, the adhesion between basal cells and the basement membrane does not recover normally (abnormal hemidesmosome reformation), and the epithelium detaches again with minor stimuli (eyelid movement during sleep or upon waking). This is recurrent corneal erosion. Corneal dystrophy and diabetes are common underlying conditions. Treatment for recurrent corneal erosion ranges from conservative therapy (lubricating eye drops, therapeutic contact lenses) to surgical interventions (diamond burr polishing, anterior stromal puncture, excimer laser PTK) [3,4].
In PED, epithelial regeneration is impaired by one or more of the following mechanisms.
Depletion of epithelial stem cells: In stem cell exhaustion (Stevens-Johnson syndrome, GVHD, chemical trauma, etc.), limbal epithelial stem cells are destroyed or depleted, leading to loss of the source of epithelial cells.
Tear film abnormalities: Severe dry eye or lagophthalmos reduces the quantity and quality of tears, worsening the ocular surface environment and impairing epithelial regeneration.
Decreased trophic factors due to sensory nerve damage: In trigeminal nerve palsy, neurotrophic factors (substance P, nerve growth factor, etc.) released from nerve endings are reduced, impairing epithelial cell proliferation and survival.
Drug toxicity: Aminoglycosides, oxybuprocaine, diclofenac sodium, etc., have direct corneal epithelial toxicity and inhibit epithelial regeneration.
Nerve growth factor (cenegermin) eye drops: Recombinant human nerve growth factor (cenegermin) eye drops, applying the component of centipede, have been reported effective for neurotrophic keratopathy. This treatment is expected to restore corneal sensation and promote epithelial healing.
Autologous serum eye drops: For PED due to neurotrophic keratopathy or GVHD, autologous serum eye drops diluted from the patient’s own serum are considered effective in promoting epithelial regeneration. EGF and nerve growth factors contained in the serum are thought to promote epithelial cell proliferation and migration.
Yu CW, Kirubarajan A, Yau M, Armstrong D, Johnson DE. Topical pain control for corneal abrasions: A systematic review and meta-analysis. Acad Emerg Med. 2021;28(8):890-908. PMID: 33508879. https://pubmed.ncbi.nlm.nih.gov/33508879/
Watson SL, Leung V. Interventions for recurrent corneal erosions. Cochrane Database Syst Rev. 2018;7(7):CD001861. PMID: 29985545. https://pubmed.ncbi.nlm.nih.gov/29985545/
Thia ZZ, Ho YT, Shih KC, Tong L. New developments in the management of persistent corneal epithelial defects. Surv Ophthalmol. 2023;68(6):1093-1114. PMID: 37301520. https://pubmed.ncbi.nlm.nih.gov/37301520/
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}