Corneal foreign body is a common condition encountered in ophthalmic emergencies. The types of foreign bodies are diverse, including metal fragments such as iron filings, glass fragments, plant matter (leaves, thorns, wood chips), stone dust, and soil. In ophthalmology outpatient clinics in metalworking areas, corneal foreign bodies account for 7.0% of new patients. According to US emergency department statistics, among urgent ophthalmic visits, external eye foreign bodies account for 7.5%, making it the second most common condition after corneal abrasion4.
88% of corneal foreign bodies are iron filings. Most foreign bodies entering the palpebral fissure are expelled by blinking, but tiny foreign bodies measuring 0.5 mm in width and 0.02 mm or less in thickness remain on the cornea. Iron rusts onto the epithelium within 30 minutes and becomes fixed on the cornea despite blinking. Corneal foreign bodies are the second most common type of ocular trauma after corneal abrasion, reportedly accounting for 30–40% of emergency ophthalmic visits 1.
Type of foreign body
Frequency
Male-to-female ratio
Iron filings
88%
27:1
Plant matter
3%
—
Sand/pebbles
2%
—
Charcoal/ash
2%
—
Other
5%
7:1
For foreign bodies other than iron filings, the male-to-female ratio is 7:1, which is less pronounced than for iron filings but still shows a male predominance. The number of foreign bodies is proportional to the width of the palpebral fissure, and they tend to be smaller at the center of the cornea and larger at the periphery.
The goal of treatment is to remove the foreign body and promote healing of the wound without complications. The condition changes depending on the type of foreign body and the time elapsed; particularly for deep corneal foreign bodies or those involving perforation, attention must be paid to the risk of infection.
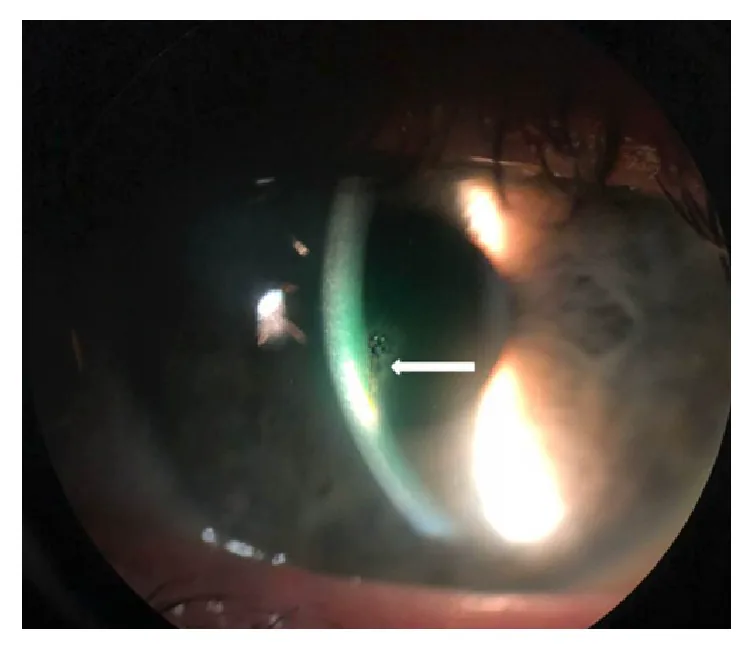
Soon AK, Mather R. Chronic, Stromal Foreign Body of Presumed Human Origin, following Corneal Abrasion. Case Rep Ophthalmol Med. 2019;2019:9607282. Figure 1. PMCID: PMC6444229. License: CC BY.
Slit-lamp photograph showing a single embedded foreign body in the central cornea with surrounding stromal haze. It gives a clear visual example of the target lesion discussed in the article.
Foreign bodies enter the eye during work or outdoor activities, causing the following symptoms.
Acute Symptoms
Eye pain: Occurs immediately after the foreign body penetrates the cornea. Severity depends on the size and depth of the foreign body.
Foreign body sensation: The foreign body on the cornea causes irritation with each blink. This persists even after removal until the epithelial defect heals.
Redness: Accompanied by conjunctival injection. In cases of severe inflammation, ciliary injection may also be observed.
Tearing: Reflex tearing due to trigeminal nerve stimulation of the cornea.
Symptoms in Prolonged Cases
Decreased vision: Foreign bodies in the pupillary area or rust rings affecting the visual axis can impair vision. Deep foreign bodies may cause irreversible visual dysfunction.
Photophobia: Occurs when complicated by anterior chamber inflammation or iridocyclitis.
Discharge: Observed when complicated by infectious keratitis.
The following findings are confirmed by slit-lamp microscopy.
Corneal foreign body: Assess the type, location, number, size, and depth of the foreign body. Iron foreign bodies appear brown to black.
Rust ring: A brown ring-shaped deposit that forms around an iron foreign body. It forms in a cylindrical shape in the epithelial layer and Bowman’s layer.
Corneal infiltration: Inflammatory cell infiltration around the foreign body. When complicated by infection, a stromal abscess may form.
Coats white ring: A small white ring-shaped opacity that remains after removal of an iron foreign body. It is due to iron deposition and usually does not require treatment.
Anterior chamber inflammation: Observed when the foreign body reaches deep layers or is left in place for a long time.
Fluorescein staining is essential for confirming epithelial damage. Disruption of the tear film around the foreign body is highlighted by staining, helping to detect transparent or very small foreign bodies. If aqueous humor leakage is present, a Seidel test can confirm perforation.
QDoes the rust ring need to be completely removed?
A
It is acceptable if complete removal is not achieved during the initial procedure. After a few days, the corneal tissue melts and the rust ring becomes easier to remove, so removal can be performed in multiple sessions. However, if the rust ring extends into the pupillary area, the condition of the stroma after removal significantly affects visual function, so careful management is required.
Corneal foreign bodies are common among workers in metal, wood, and plastic manufacturing, construction, agriculture, and cleaning industries. In daily life, do-it-yourself projects, gardening, and cleaning can also be triggers. A study of ocular trauma cases in the emergency department found that 83% of patients were male, mean age 34 years, 72.1% were work-related, and the main types of foreign bodies were metal fragments (37.6%) and dust (31.1%) 5. Inquiring about the circumstances of injury and inferring the type of foreign body helps determine the treatment strategy.
Iron filings: Rust within 30 minutes, forming a cylindrical rust ring within 12 hours. After 72 hours, the area around the rust ring dissolves, but infection is unlikely.
Plant material (thorns, wood chips): Causes a strong foreign body reaction in the corneal stroma. Over time, swelling and decay progress, and bacteria or fungi can invade the cornea, easily causing infectious keratitis. Cases of fungal keratitis caused by Aspergillus species after corneal foreign bodies of iron or organic matter have been reported, and some cases became apparent after long-term eye drop use 3.
Chestnut burrs or caterpillar venomous hairs: Can cause severe visual impairment due to contained toxins. Venomous hairs may also invade the vitreous cavity.
Sharp foreign bodies (glass, metal fragments): May penetrate deep into the cornea and cause perforation.
QWhy are plant-based foreign bodies particularly dangerous?
A
Plant-based foreign bodies cause a strong foreign body reaction within the corneal stroma. Over time, they swell and decompose, leading to fragmentation and retention. Additionally, plants often carry bacteria and fungi, increasing the risk of infectious keratitis. Steroid eye drops are contraindicated because they promote fungal infection.
At the first visit, do not force the eyelid open; use topical anesthetic eye drops to reduce irritation before examination. Handle carefully, considering the possibility of perforating injury.
History: Assess the circumstances of injury, estimate the type of foreign body, and determine the time elapsed since injury.
Slit-lamp examination: Identify the type, location, number, size, and depth of the foreign body. Also evaluate for anterior chamber inflammation and iridocyclitis.
Fluorescein staining: Assess the extent of epithelial damage. Perform Seidel test to determine the presence of perforation.
Fundus examination: If an intraocular foreign body is suspected, use an auxiliary lens to observe from the posterior pole to the far periphery.
Imaging Studies (When Deep or Intraocular Foreign Body Is Suspected)
X-ray examination: Useful for confirming and locating the foreign body. If an intraocular foreign body is found, confirm its position using the Comberg method.
CT scan: Performed when X-ray is difficult to detect. It can also evaluate changes in the orbit and cranium simultaneously.
Ultrasound: Useful when the fundus cannot be visualized due to anterior segment opacity or vitreous hemorrhage. It is also used to search for foreign bodies that cannot be detected by X-ray, such as glass or plastic.
MRI: Can only be performed when the foreign body is clearly non-magnetic. It is absolutely contraindicated if a magnetic foreign body is suspected.
Eye irrigation may be effective for powdery or granular foreign bodies on the ocular surface. However, foreign bodies that are embedded or stuck in the cornea cannot be removed by irrigation. An ophthalmologist must thoroughly examine the anterior segment with a slit lamp and select the appropriate treatment.
After topical anesthesia, the following procedures are performed under a slit lamp. Removal is standardly performed using a sterile needle or burr (drill) under topical anesthesia 12.
Basic Technique for Foreign Body Removal
Removal with a foreign body spud: Use the spud like a scalpel, sharp spoon, or spatula to lift and remove the foreign body. Do not direct the tip perpendicular to the cornea.
27G needle method: Lift and remove the foreign body with a disposable injection needle. Foreign bodies other than iron filings are often just resting on the cornea and can be removed by scooping.
Removal with forceps: Grasp the posterior end of the foreign body with jewelers forceps and pull it out. Be careful not to disturb the surrounding tissue.
Removal of Rust Ring
Curettage with a foreign body spud: After removing the epithelial rust ring, scrape out the punctate rust remaining in the superficial stroma with the tip of the spud.
Curettage with a drill (Alger brush): Compared to the spud technique, there is less residual rust after the first attempt. Adjust the drill to low speed and lightly touch the tip to avoid over-scraping.
Stepwise removal: Even if complete removal is not possible at the first attempt, removal can be performed again after a few days when the corneal tissue has softened.
Removal of deep foreign bodies or those with perforation
This is performed under a surgical microscope with an eyelid speculum in place.
Incision + forceps extraction: An incision is made at the entry site of the foreign body with a scalpel, and the foreign body is removed with forceps.
30G needle technique: The needle tip is inserted around the foreign body through the incision, and the foreign body is extracted by lifting it up.
Foreign body reaching the anterior chamber: Retrobulbar anesthesia is administered to suppress eye movement before removal. There are two approaches: corneal side and anterior chamber side.
Anterior chamber approach: The anterior chamber is maintained with viscoelastic material, the foreign body is pulled into the anterior chamber with anterior capsule forceps, and then removed from the eye through a side port.
Management of perforation wound: Small fresh wounds can be expected to self-seal. Large wounds are sutured with 10-0 nylon.
After foreign body removal, the wound site has a disrupted epithelial barrier function and is susceptible to infection.
Antibiotics: Apply antibiotic eye ointment and administer antibiotic eye drops early after surgery. Standard care after removal includes antibiotics, lubricants, and cycloplegics as needed for infection prevention, along with close follow-up until epithelial regeneration is confirmed12.
Sodium hyaluronate eye drops: Used in combination for corneal epithelial regeneration and protection.
Steroid eye drops: Generally not used, as they promote an infection-prone environment and mask signs of infection. Especially contraindicated after vegetable foreign bodies to prevent fungal infection3.
Atropine eye ointment: Used as an anti-inflammatory adjunct when anterior chamber inflammation is severe.
Follow-up: Carefully observe for several days postoperatively until robust corneal epithelium regenerates and barrier function recovers. According to primary care literature, if appropriate evaluation and removal techniques are mastered, many cases can be managed on an outpatient basis, and only cases with deep foreign bodies, perforation, or infection should be referred to a specialist26.
QWhich is more suitable for rust ring removal: a drill or a foreign body needle?
A
The drill (Alger brush) has the advantage of fewer initial remnants compared to the foreign body needle. However, it has the disadvantage of potentially over-removing stromal tissue. It is important to use low speed and lightly touch the tip. Especially for rust rings involving the pupillary area, careful consideration of indications is necessary because the condition of the stroma after removal affects visual function.
When iron particles adhere to the cornea, oxidation progresses in the presence of moisture and oxygen. Rusting of the epithelium occurs within 30 minutes, and a cylindrical rust ring forms in the epithelial layer within 12 hours. Rust reaching Bowman’s layer spreads in a disc shape proportional to the volume of iron particles, and further forms a cylindrical rust ring in the superficial stroma directly beneath. After 72 hours, the tissue surrounding the rust ring begins to dissolve, but infection usually does not occur at this stage.
A small white ring-shaped opacity that remains in the corneal stroma after removal of an iron foreign body. It is an iron deposit that remains as a trace of the foreign body in the cornea. Usually asymptomatic and does not require treatment; it may regress over time.
Disruption of the epithelial barrier by corneal foreign bodies provides a route for bacterial and fungal invasion. Organic foreign bodies carry microorganisms into the corneal stroma, posing a particularly high risk of infection. If not properly treated, it can progress from corneal ulcer to iridocyclitis and panophthalmitis, significantly impairing visual function.
For inert foreign bodies such as glass fragments that are difficult to remove, if they do not affect vision and cause no chemical or physical irritation, observation may be acceptable. However, follow-up is necessary.
Channa R, Zafar SN, Canner JK, Haring RS, Schneider EB, Friedman DS. Epidemiology of Eye-Related Emergency Department Visits. JAMA Ophthalmol. 2016;134(3):312-319. PMID: 26821577. https://pubmed.ncbi.nlm.nih.gov/26821577/
Yiğit O, Yürüktümen A, Arslan S. Foreign body traumas of the eye managed in an emergency department of a single-institution. Ulus Travma Acil Cerrahi Derg. 2012;18(1):75-79. PMID: 22290055. https://pubmed.ncbi.nlm.nih.gov/22290055/