Acid burn is a disease in which the cornea and conjunctiva are damaged when acidic chemicals enter the eye. It is an ophthalmic emergency requiring immediate response.
The incidence of ocular chemical trauma is estimated at 65–78 per 100,000 population1). The average age is 48 years. Although alkali injuries are more common than acid injuries, acid burns also occur at a certain rate as occupational injuries1).
The most common causative agents are hydrochloric acid (toilet cleaner, industrial chemicals), sulfuric acid (battery fluid), and nitric acid (industrial chemicals). They occur in a wide range of settings, from household accidents (misuse of toilet cleaner) to occupational exposure in factories and research facilities.
Acidic agents have low tissue permeability, so damage often remains superficial. In contrast, alkalis dissolve proteins and reach the deep cornea, causing deep damage in a short time and leading to complications such as severe stromal opacity, endothelial damage, cataract, iritis, and glaucoma.
Causative agent
Main uses/exposure situations
Characteristics
Hydrochloric acid
Toilet cleaner, industrial chemicals
Volatile
Sulfuric acid
Battery acid, industrial chemicals
Strong acid, risk of severe injury
Nitric acid
Industrial chemicals, research facilities
Oxidizing
Hydrofluoric acid
Glass etching, semiconductors
Highly penetrating, especially severe
QAre acid injuries milder than alkali injuries?
A
In general, acid burns tend to remain more superficial than alkali burns and often have a better prognosis. This is because acids coagulate proteins, forming a self-protective barrier that limits depth of penetration. However, strong acids such as sulfuric acid and hydrofluoric acid can penetrate deeply, causing severe damage similar to alkali. Severity depends on the type of substance, pH, concentration, and contact time.
Characteristic findings of acid burns include white deposits due to coagulation necrosis and relatively preserved conjunctival injection. In alkali injuries, liquefactive necrosis leads to ischemia, often resulting in white edema without injection.
Acid Burns
Injection pattern: coagulation necrosis tends to preserve conjunctival injection
Depth of injury: a self-protective barrier forms due to protein coagulation, often limiting damage to superficial layers
Exceptions with strong acids: sulfuric acid and hydrofluoric acid can penetrate deeply
Alkali Injuries
Injection pattern: saponification → liquefactive necrosis → ischemia leads to white edema without injection
Depth of injury: no barrier forms; rapid penetration into deep corneal stroma and anterior chamber
Complications: prone to iritis, cataract, and secondary glaucoma
Fluorescein staining confirms the corneal epithelial defect. When the corneal and conjunctival epithelium is extensively damaged, the entire area may stain uniformly and faintly, making it appear as if there is no epithelial defect, so caution is required.
Severe acid burns can also cause iritis, secondary glaucoma, and symblepharon.
QWhy does the conjunctiva not turn white in acid injury?
A
Acid coagulates tissue proteins (coagulation necrosis), so ischemia that occludes blood vessels is relatively less likely to occur, and conjunctival hyperemia tends to be preserved. In contrast, alkali saponifies and liquefies cell membrane lipids, causing extensive destruction of tissues including blood vessels, leading to white edema lacking hyperemia due to ischemia. However, strong acids can cause extensive tissue necrosis and may also result in ischemia.
The severity of acid burns is determined by the following factors.
Type of agent: Strong acids such as hydrofluoric acid and sulfuric acid tend to cause severe injury
pH: Lower pH results in greater damage
Concentration: Higher concentration leads to deeper tissue involvement
Contact time: Time until irrigation is the greatest determinant of prognosis
Area of exposure: Widespread exposure tends to cause severe injury
Hydrofluoric acid has particularly high penetrability and causes extensive destruction of the cornea, sclera, and anterior segment. Caution is needed for occupational exposure (glass etching, semiconductor manufacturing).
Occupational exposure (factories, chemical research facilities) is most common, but it also occurs in household accidents (toilet bowl hydrochloric acid cleaners, battery acid).
Immediately after injury, measure the pH of tears with pH test paper. In acid burns, the pH is low (acidic). Perform irrigation until the pH becomes neutral (pH 7–7.2).
In acid burns, the pH tends to normalize quickly after irrigation (faster normalization compared to alkali). However, residual acid in the tissue may be released, so it is important to recheck the pH 20 minutes after irrigation.
The Kinoshita classification evaluates severity based on the extent of remaining POV (palisades of Vogt), the site of limbal epithelial stem cells, and is useful for prognosis.
Limbus conjunctival necrosis over half circumference, total corneal epithelial defect, complete POV loss
Poor
The Roper-Hall classification is a 4-grade system based on the degree of corneal opacity and the extent of limbal ischemia. The Dua classification further subdivides Roper-Hall Grade IV into three stages according to the proportion of limbal and conjunctival involvement, enabling more precise prognosis assessment 1).
Detailed history of injury (type of substance, pH confirmation)
Eye irrigation (until pH is near neutral)
Slit-lamp examination and fluorescein staining
Severity assessment using the Kinoshita classification
Visual acuity, intraocular pressure, and fundus examination
QWhat is the difference between diagnosing acid injury and alkali injury?
A
The main difference is the rate of pH change. In acid burns, the pH tends to neutralize quickly after irrigation, so the clinical appearance may seem mild. However, residual acid in the tissue can cause the pH to drop again, so pH must be rechecked 20 minutes after irrigation. The severity classification and examination flow are the same as for alkali injuries.
Regardless of the chemical type, starting irrigation as soon as possible is most important. Time to irrigation and volume of irrigant are the greatest factors determining prognosis. Irrigation should be performed for at least 20 minutes, and continued as long as possible.
At the scene, immediately start irrigation with running tap water. At the ophthalmology clinic, after topical anesthesia, thoroughly irrigate the conjunctival sac with saline (isotonic solution preferred), and recheck pH 20 minutes after irrigation.
For mild to moderate injuries (Kinoshita classification Grade 1–2), topical antibiotics and steroid eye drops/ointments are prescribed to control infection and inflammation. For more severe injuries, systemic steroids are administered intensively for about one week and then tapered.
Topical antibiotics: New quinolone antibiotics for infection prevention
For Grade 3b or higher, or when severe limbal ischemia is present, acute surgical treatment is added.
Tenon’s capsule plasty is a procedure that advances the Tenon’s capsule to the limbus to restore blood supply in cases of limbal and scleral ischemia, and is useful as an eye-preserving surgery in severe chemical trauma2).
In the cicatricial phase, ocular surface reconstruction is performed using a combination of limbal stem cell transplantation (autologous or allogeneic), amniotic membrane transplantation, and full-thickness corneal transplantation. For severe bilateral cases, femtosecond laser-assisted large-diameter lamellar keratolimbal transplantation has been applied, with reports of good visual improvement3).
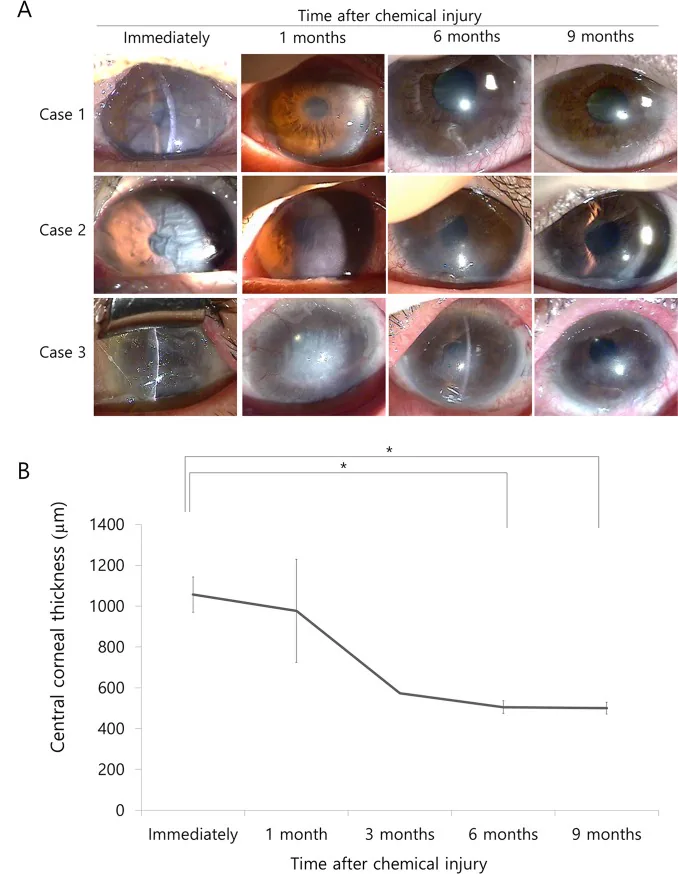
Choi SO, Jeon HS, Hyon JY, et al. Recovery of Corneal Endothelial Cells from Periphery after Injury. PLoS One. 2015;10(9):e0138076. Figure 1. PMID: 26378928; PMCID: PMC4574742; DOI: 10.1371/journal.pone.0138076. License: CC BY.
Anterior segment photographs (3 cases) from immediately after chemical burn (Immediately) to 1, 6, and 9 months later. Immediately after injury, all cases show severe corneal edema, opacity, and Descemet’s membrane folds, with loss of endothelial cells. Over time, clearing progresses from the periphery, and corneal opacity eventually decreases. This corresponds to corneal damage due to coagulation necrosis and its recovery process discussed in the section “Pathophysiology and detailed pathogenesis.”
Acidic substances denature and coagulate tissue proteins (coagulation necrosis), forming insoluble proteins. This coagulated protein acts as a barrier (self-protective membrane), limiting further penetration of the acid. Therefore, damage is often limited to the superficial layers compared to alkali injuries.
However, changes in ocular surface pH and residual acid in the tissue cannot be overlooked. Hydrofluoric acid has particularly high penetrability, causing extensive destruction of the cornea, sclera, and anterior segment. Strong acids (such as high-concentration sulfuric acid) can cause deep damage and may penetrate into the anterior chamber.
Alkali saponifies cell membrane lipids with hydroxyl ions, causing liquefactive necrosis. Being lipophilic, it easily passes through the epithelial layer and penetrates deep into the stroma within a short time. Alkali that penetrates into the anterior chamber causes iritis, cataract, and glaucoma.
In contrast, coagulation necrosis caused by acid relatively preserves tissue structure, and acute hyperemia tends to be maintained. However, if limbal corneal and conjunctival epithelial stem cells are damaged, regeneration of transparent corneal epithelium becomes difficult, and conjunctival epithelium invades the cornea (conjunctivalization). Limbal ischemia increases the risk of limbal stem cell deficiency (LSCD), leading to corneal scar formation and permanent visual impairment2).
The course after chemical injury is classified into acute, early reparative, and late reparative phases. In the acute phase, damage to the corneal and conjunctival epithelium and inflammation occur. In the early reparative phase, epithelial regeneration and inflammatory reactions proceed in parallel. In the late reparative phase, scar formation, symblepharon, and conjunctival sac shortening occur, worsening the ocular surface environment.
AS-OCTA enables objective quantification of limbal ischemia in the acute phase of chemical injury, providing more accurate severity assessment and prognosis prediction than clinical evaluation. AS-OCTA results correlate well with final visual outcomes, and integration into existing classification systems is expected2).
Femtosecond laser-assisted large-diameter lamellar corneal limbal transplantation can simultaneously transplant corneal stroma and limbal stem cells as a one-stage surgery for severe bilateral chemical trauma. Compared to conventional manual dissection, it enables uniform lamellar dissection, and good visual improvement has been reported3).
The application of femtosecond laser is limited in the number of cases, and further research is needed to establish long-term efficacy3). Standardization of AS-OCTA and its incorporation into classification systems remain future challenges2).
Chemical injuries of the eye. Ann Eye Sci. 2023;8:13.
Sharma S, Kate A, Donthineni PR, Basu S, Shanbhag SS. The role of Tenonplasty in the management of limbal and scleral ischemia due to acute ocular chemical burns. Indian journal of ophthalmology. 2022;70(9):3203-3212. doi:10.4103/ijo.IJO_3148_21. PMID:36018089; PMCID:PMC9675520.
Lin L, Xu Y, Ou Z, Zhuo K, Tian D, Chen J, et al. Femtosecond laser-assisted large-diameter lamellar corneal-limbal keratoplasty in ocular chemical burns. American journal of ophthalmology case reports. 2025;37:102246. doi:10.1016/j.ajoc.2024.102246. PMID:39839915; PMCID:PMC11745959.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.