Terrien’s marginal degeneration (TMD) is a rare degenerative disease characterized by peripheral corneal stromal thinning with lipid deposition and superficial neovascularization. It is slowly progressive, typically non-inflammatory, and follows a bilateral and asymmetric course. In the early stage, arcuate fine granular stromal opacities appear in the peripheral cornea, leaving a clear zone between the opacity and the limbus. As it progresses, the edge of the thinned area becomes scalloped like a shell, accompanied by lipid deposits and pseudopterygium. When thinning becomes marked, the corneal stroma weakens and protrudes forward, causing visual impairment due to high against-the-rule astigmatism or irregular astigmatism.
This disease was first described in 1900 by the French ophthalmologist Louis-Auguste Terrien, and for over a century it has been regarded as a representative example of peripheral corneal degeneration characterized by stromal thinning. The exact prevalence is unknown, but it is rare worldwide, and even corneal specialists encounter only a limited number of cases in their lifetime. Progression is generally slow, and symptoms may not become apparent for several years to decades. However, in advanced stages, against-the-rule astigmatism can interfere with reading and driving, and rarely, perforation may occur. Therefore, long-term follow-up and timely intervention are important.
Onset is most common after the age of 40, with a slight male predominance. The male-to-female ratio is reported to be approximately 3:1, mainly in the 20s to 40s, with a bimodal distribution of typical middle-aged/elderly cases and juvenile-onset cases 4). In a multicenter case series of 25 patients by Chan et al., 28% (7 cases) were unilateral, revising the conventional wisdom that the disease is “principally bilateral” 3). The youngest reported case is a 6-year-old girl 5), and Mandal et al. reported in detail a case of unilateral TMD in a 10-year-old boy 2).
Two clinical types are known.
Clinical type
Characteristics
Typical middle-aged and elderly type
Asymptomatic, slowly progressive, non-inflammatory, bilateral and asymmetric
Juvenile-onset type
More common in men in their 20s-30s, associated with recurrent episcleritis and anterior segment inflammation13)
Thinning usually begins superiorly, presenting with mild punctate subepithelial opacities and anterior stromal opacities. A clear area remains between the opacity and the limbus. Following the opacity, fine vascular pannus develops in the peripheral superficial layer and extends circumferentially over several years to decades. A yellowish-white line due to lipid deposition appears at the leading edge, and blood vessels cross the groove and extend beyond it. Thinning is more common superiorly but can occur in any direction. It rarely extends to the inferior limbus. During the course, the corneal epithelium characteristically remains intact.
Approximately 20% of cases have associated pseudopterygium. Spontaneous perforation is rare, but attention should be paid to the fact that perforation can easily occur with minor trauma. In Chan et al.’s series, corneal perforation was observed in 5 of 25 eyes, of which 4 were spontaneous perforations3).
QDoes TMD occur in children?
A
TMD usually develops in the 20s to 40s, but several cases of childhood onset have been reported. The youngest case was a 6-year-old girl with corneal thinning from 4 to 8 o’clock inferiorly5). Mandal et al. reported unilateral TMD in a 10-year-old boy with arcuate stromal thinning from 9 to 3 o’clock superiorly, with lipid deposition and neovascularization2). In children, there is a high risk of amblyopia due to irregular astigmatism, so early refractive correction and regular follow-up are important2). Spontaneous perforation can also occur in children, so the risk of perforation should be explained and careful follow-up is needed14).
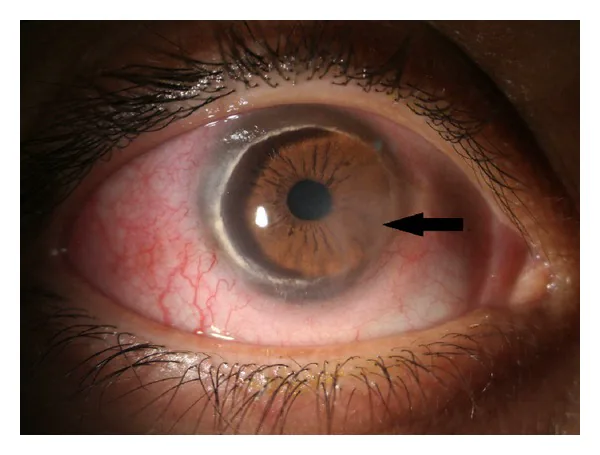
Vejdani AH, et al. Partial and Total Descemet’s Detachments in a Patient with Severe Terrien’s Marginal Degeneration and Juvenile Idiopathic Arthritis. Case Reports in Ophthalmological Medicine. 2014;2014:279491. Figure 1. PMCID: PMC4131067. License: CC BY.
Slit-lamp photograph of the right eye. A ring-shaped thinning groove, opacity, lipid deposition, and neovascularization are seen in the peripheral cornea. The image shows lipid deposition and neovascularization overlapping the thinning lesion that progresses predominantly in the periphery.
Blurred vision: The most common symptom, gradually worsening with progression of against-the-rule astigmatism. Typically painless.
Asymptomatic course: In mild cases, there may be no subjective symptoms other than astigmatism. Often discovered incidentally during health checkups or treatment of other diseases.
Foreign body sensation and pain: In juvenile-onset type, recurrent episodes of pain and conjunctival injection may occur 13).
Acute vision loss: Perforation after minor trauma can cause sudden vision loss and pain 3)15).
Clinical Findings (Findings Confirmed by Physician Examination)
Peripheral corneal thinning: Usually begins superiorly, forming a crescent- or arcuate-shaped gutter. The central wall is steep, while the peripheral side slopes gently. The margin is scalloped like a shell.
Clear zone: In early stages, a 1–2 mm clear area remains between the opacity and the limbus.
Lipid deposition: Yellow-white linear lipid deposits at the central edge of the gutter (tip of pannus). Vessels cross the gutter and extend beyond the deposits.
Superficial neovascularization (pannus): Fine vessels extend from the limbus toward the thinned area. Typically progresses quietly without limbal inflammation.
Pseudopterygium: Occurs in about 20% of cases.
Epithelial integrity: The corneal epithelium remains intact and does not stain with fluorescein. This is a key difference from Mooren’s ulcer and peripheral ulcerative keratitis.
High against-the-rule astigmatism: Progressive flattening of the vertical meridian causes high against-the-rule or irregular astigmatism. In a 10-year-old boy reported by Mandal et al., 6.3 D of against-the-rule astigmatism was noted, and spectacle correction (-6 DC at 90°) improved visual acuity from 20/200 to 20/60 2).
Atypical findings: In juvenile-onset type with conjunctival injection and episcleritis, thinning progresses with recurrent anterior segment inflammatory episodes 13).
AS-OCT findings: A subepithelial hyperreflective band may be observed around the thinned area, indicating potential subclinical inflammation even when clinically non-inflammatory 2)6). In Mandal et al.’s case, corneal thickness at the thinnest area was 305 μm temporally and 355 μm nasally 2). Serial corneal thickness measurements are important for assessing progression; a case with a 15 μm decrease over one year has been reported 2).
The main cause of vision loss is high-degree irregular astigmatism. When correctable with glasses, interference with daily life is mild, but when irregular astigmatism becomes prominent, higher-order aberrations increase, and patients become aware of image distortion and ghosting even with glasses. Decreased night vision, photophobia, and reduced contrast sensitivity are also typical complaints in advanced stages. In bilateral, asymmetric progression, the refractive difference between the eyes increases, which can lead to aniseikonia. In pediatric cases, if high irregular astigmatism occurs during the critical period of visual development, it can lead to irreversible amblyopia; therefore, early refractive correction and amblyopia training are crucial for prognosis 2).
The etiology remains unknown. Currently, two hypotheses coexist: a degenerative origin and an inflammatory origin 4). Histologically, defects in Bowman’s membrane, rupture of Descemet’s membrane, and formation of intra-stromal cysts are observed. Light microscopy shows subepithelial fibrous collagen degeneration, and electron microscopy reveals collagen precursors, stromal matrix, and phagocytosis of lipids by histiocytes with high lysosomal activity 4). The lysosomal activity of histiocytes is thought to be involved in the destruction of collagen fibers. In juvenile-onset cases, inflammatory cell infiltration around vascular invasion has been reported, suggesting involvement of immune-mediated mechanisms 13). No clear hereditary pattern has been established, and familial cases are extremely sporadic. No strong association with specific systemic diseases is known, but reports of coexistence with keratoconus and PPCD (described below) suggest a common basis of corneal structural vulnerability.
Coexistence with keratoconus: Pouliquen et al. reported cases where TMD and keratoconus occurred in the same eye or in both eyes of the same patient 7).
Subclinical corneal shape abnormality in the fellow eye: Nahata et al. reported a woman in her 20s with unilateral TMD whose fellow eye was clinically normal (visual acuity 20/20) but showed inferior steepening and posterior elevation on corneal topography, indicating keratoconus-like topographic changes 1). This suggests a link between TMD and the corneal ectasia spectrum.
Coexistence with anterior basement membrane dystrophy, persistent erythema elevatum diutinum, etc., has also been sporadically reported.
Vasculitis-related: Keenan et al. reported a case of asymmetric development of Fuchs superficial peripheral keratitis and TMD associated with vasculitis 16).
In advanced TMD, the corneal stroma is markedly thinned, so even minor trauma can cause corneal perforation. In Chan et al.’s case series, perforation was observed in 5 of 25 eyes 3). Chung et al. reported spontaneous perforation in pediatric cases 14), and Srinivasan et al. in adult cases 15).
The diagnosis of TMD is clinical, and slit-lamp examination is most useful. Corneal topography and anterior segment optical coherence tomography (AS-OCT) increase diagnostic accuracy and contribute to evaluation of the inflammatory phase and differential diagnosis. In 2021, the Nordic Terrien degeneration study proposed diagnostic criteria based on peripheral thinning with lipid deposition, superficial neovascularization, and epithelial integrity 9).
Slit-Lamp Examination
Basic findings: Confirm the leading edge of lipid deposition, a steep central edge and a gentle peripheral edge, intact epithelium, and superficial neovascularization extending from the limbus to the thinned area.
Advanced findings: Systematically observe findings that differentiate from Mooren’s ulcer and rheumatoid peripheral ulcer, such as pseudopterygium (in about 20%), a shell-like fan-shaped margin, and preservation of anterior chamber depth.
Fluorescein staining: Usually not stained. If stained, it suggests severe thinning or impending perforation.
Corneal Topography and AS-OCT
Reverse crab claw pattern: Flattening of the thinned peripheral cornea and relative steepening of the cornea approximately 90 degrees away from the midpoint 1)2). While the crab claw pattern of pellucid marginal degeneration (PMD) is located inferiorly, in TMD it is located superiorly, hence termed “reverse” 2).
Quantitative evaluation of against-the-rule astigmatism: In Mandal et al.’s case, 6.3 D of against-the-rule astigmatism was detected 2). Useful for tracking changes over time.
AS-OCT evaluation of inflammatory phase: In the quiescent phase, only localized stromal thinning is seen, but in the inflammatory phase, a hyperreflective subepithelial band appears adjacent to the thinned area 6). It can detect potential inflammatory phases even when clinical signs of inflammation are absent 2).
Evaluation of the contralateral eye: Nahata et al. reported that even clinically normal contralateral eyes showed irregular patterns (keratoconus-like changes) on corneal topography, emphasizing the need for systematic evaluation of the contralateral eye even in cases that appear unilateral1).
The main diseases that require differentiation from TMD are listed below2)4). The presence or absence of lipid deposition, epithelial defects, pain/inflammation, and the predilection site of thinning are key points for differentiation.
Disease
Differentiating points from TMD
Mooren’s ulcer
Severe pain/inflammation, epithelial defect present, overhanging edge, no lipid deposition
Local dehydration at tear film breakup, occurs adjacent to pterygium or filtering bleb
Juvenile-onset TMD is accompanied by scleritis and anterior segment inflammation, so in atypical cases, differentiation from Mooren’s ulcer and collagen disease-related PUK is particularly important 13). Blood tests for screening collagen diseases and vasculitis (antinuclear antibody, rheumatoid factor, ANCA, HLA-B27, syphilis serology, etc.) may be necessary. In the case of Mandal et al., after testing all of HLA-B27, c-ANCA, p-ANCA, antinuclear antibody, rheumatoid factor, anti-CCP antibody, HBs antigen, HCV, HIV, etc., and confirming negativity, the diagnosis of TMD was established 2).
The clinical key points for differential diagnosis are summarized below. First, presence of pain and epithelial defect: if neither is present, TMD or senile furrow degeneration is likely. Second, presence of lipid deposition: yellowish-white linear deposits at the advancing edge strongly suggest TMD. Third, predilection site of thinning: superior predominance suggests TMD, inferior predominance suggests PMD, and circumferential involvement suggests PUK. Fourth, nature of neovascularization: fine superficial pannus extending quietly from the limbus to the thinned area is characteristic of TMD, and is distinguished from the vascular reaction with active inflammation in Mooren’s ulcer.
QShould the contralateral eye of TMD also be evaluated?
A
It should definitely be evaluated. Nahata et al. reported corneal topographic changes such as inferior steepening and posterior elevation in the clinically normal contralateral eye (visual acuity 20/20) of a woman in her 20s with TMD in the right eye, indicating keratoconus-like topographic changes 1). Even in cases considered unilateral TMD, there is a possibility of latent corneal shape abnormalities or changes belonging to the corneal ectasia spectrum in the contralateral eye. Follow-up with topography at the initial visit and at least once a year is recommended 1).
TMD is slowly progressive and typical cases are asymptomatic, so the basis of treatment is observation and refractive correction. Active intervention is necessary when inflammatory attacks or impending perforation occur.
Observation: Asymptomatic typical cases do not require treatment; monitor progression with slit-lamp examination and corneal topography every 6 months to 1 year. The rate of progression varies greatly among individuals; some cases remain almost stationary for decades, while others progress to high against-the-rule astigmatism within a few years.
Spectacle correction: First choice for astigmatism. Mild to moderate against-the-rule astigmatism can be managed with glasses. Update the prescription with regular refraction examinations.
Oxygen-permeable hard contact lenses (RGP-CL) and scleral lenses: For high irregular astigmatism that is difficult to correct with glasses, correction with RGP-CL or scleral lenses is attempted 4). Scleral lenses span the entire cornea and adjust refraction through the tear film, reducing aberrations caused by irregular peripheral shape changes, and are easier to apply in advanced TMD. However, tolerance to contact lenses is often low in elderly patients, and fitting may be difficult in children 2).
Lubricating eye drops: Artificial tears such as carboxymethylcellulose 0.5% are used for surface irregularities. In a pediatric case by Mandal et al., symptom relief was reported with lubricating eye drops alone 2).
Low-concentration steroid eye drops: For inflammatory attacks with conjunctival hyperemia or episcleritis, low-concentration steroid eye drops such as fluorometholone 0.1% three times daily are used. Since long-term use may be necessary in juvenile-onset cases, attention should be paid to side effects such as intraocular pressure and posterior subcapsular cataract, and the lowest effective concentration and shortest duration should be used.
Surgery is indicated when perforation is imminent due to progressive thinning, or when visual acuity is significantly reduced due to astigmatism. The AAO Preferred Practice Pattern recommends peripheral crescentic or annular patch grafts for cases with marked peripheral stromal loss and increasing astigmatism, including TMD 11).
Crescentic patch graft: A lamellar or full-thickness corneoscleral patch graft is placed at the thinning site. It reinforces partial stromal loss and may suppress astigmatism progression long-term. Long-term reports have shown suppression of severe against-the-rule astigmatism progression for up to 20 years 4). Fernandes et al. reported good visual function after patch grafting in a case of bilateral TMD with perforation after minor trauma 12).
Annular lamellar keratoplasty: Indicated for severe cases with 360-degree peripheral degeneration 4). A donut-shaped graft is sutured around the entire limbus.
Automated lamellar therapeutic keratoplasty (ALTK): Selected for tectonic reinforcement in cases of progressive peripheral thinning 11).
Therapeutic soft contact lenses: For small perforations, temporary closure with tissue adhesive (cyanoacrylate) may be used, and surgery can be planned in a second stage.
Full-thickness penetrating keratoplasty (PK): For lesions extending to the central cornea or cases with extensive irregular astigmatism, eccentric PK or rotational autograft may be selected 11). Eccentric PK is a technique in which a circular graft is sutured shifted from the center to the periphery, allowing removal of the lesion while avoiding the pupillary zone. However, postoperative astigmatism management is difficult, and patient selection is crucial.
Postoperative management: Regardless of the surgical technique, long-term topical steroid eye drops, monitoring for suture-related infections, and evaluation of residual corneal shape are necessary. Early gradual suture removal optimizes astigmatism, and RGP-CL is reintroduced as needed.
In the lesion area of TMD, the epithelium can be normal, thickened, or thinned. Bowman’s layer is usually absent or degenerated, and Descemet’s membrane may show thinning or breaks. Intra-stromal cysts form within the affected stroma, and subepithelial fibrous collagen degeneration is observed under light microscopy. Electron microscopy reveals collagen precursors, stromal matrix, and phagocytosis of lipids by histiocytes with high lysosomal activity, suggesting that lysosomal activity of histiocytes is involved in the slow destruction of collagen fibers 4).
TMD has long been considered a non-inflammatory degenerative disease, but Austin et al. reported inflammatory TMD with juvenile onset in 1981, proposing the coexistence of degenerative and inflammatory theories 13). In a multicenter case series by Chan et al., the proportion of cases with inflammatory episodes and prognostic features were analyzed in detail, showing that the inflammatory type progresses faster and tends to require surgical intervention than the non-inflammatory type 3).
Rodriguez et al. showed that high-resolution AS-OCT can differentiate between inflammatory and non-inflammatory types of peripheral corneal thinning. In the quiescent phase, only localized stromal thinning is observed, but in the inflammatory phase, a subepithelial hyperreflective band appears adjacent to the thinning area 6). In pediatric cases by Mandal et al., despite the absence of clinical inflammatory signs, AS-OCT revealed a subepithelial hyperreflective band, suggesting a potential inflammatory phase 2). This finding is used to guide treatment decisions (indication for steroid eye drops) and predict prognosis.
In TMD, the thinned area of the cornea becomes flat, and relative steepening occurs at 90 degrees to it, resulting in strong against-the-rule astigmatism. This change is depicted as a reverse crab claw pattern on corneal topography1)2). While the crab claw pattern of PMD is located inferiorly, the lesion in TMD is often located superiorly, hence the term “reverse” 2). In advanced stages, forward protrusion of the thinned area becomes prominent, making irregular astigmatism difficult to correct.
TMD has been considered rare to cause spontaneous perforation, but in cases with marked stromal thinning in advanced stages, even minor trauma (eye rubbing, blunt trauma, contact lens insertion/removal, etc.) can easily lead to perforation. In Chan et al.’s series, perforation was observed in 5 of 25 eyes, of which 4 were spontaneous perforations without clear traumatic triggers 3). Chung et al. reported a case of spontaneous perforation in a child with TMD 14), and Srinivasan et al. reported an adult case where the initial symptom was spontaneous perforation 15). In cases where the thinned area decreases to around 100 μm, the risk of perforation increases sharply, so quantitative monitoring with AS-OCT and early surgical intervention are essential.
QHow to differentiate TMD from Mooren's ulcer?
A
TMD is painless with intact epithelium, and the advancing edge is accompanied by lipid deposition and superficial neovascularization. In contrast, Mooren’s ulcer is associated with pain and hyperemia, epithelial defects, and a characteristic “overhanging edge” at the ulcer margin. TMD often lacks anterior segment inflammation, and thinning progresses slowly over years. However, there is a juvenile subtype of TMD with inflammatory episodes 13); in atypical cases, blood tests for collagen disease/vasculitis screening and AS-OCT for inflammatory phase assessment are useful for differentiation 2)6).
The 2021 Nordic Terrien degeneration study proposed diagnostic criteria for TMD, which had not been unified previously, and formulated clinical criteria centered on lipid deposition, superficial neovascularization, and epithelial integrity 9). Standardization of diagnostic criteria is expected to facilitate multicenter case registration and prospective observational studies. High-resolution AS-OCT for differentiating inflammatory/ quiescent phases is increasingly applied to treatment decision-making and is becoming established as a means to detect latent inflammation not captured by conventional slit-lamp findings alone 6).
Scleral lenses are attracting attention as a non-invasive option for severe irregular astigmatism because they vault the central cornea and absorb the refractive influence of the peripheral thin area 4). Large-diameter RGP lenses and hybrid lenses are also options and have been actively considered in recent years as a means to avoid surgery. Peripheral corneal cross-linking (CXL) is being discussed for potential application to TMD, but many cases fall below the required corneal thickness (≥400 μm) in the thin area, so indications are limited. Bioengineered corneal grafts for tectonic reinforcement, clinical application of decellularized donor tissue, and crescent-shaped scaffolds using 3D printing may be future research subjects, but no large-scale randomized controlled trials for TMD currently exist, and current evidence relies on case series and retrospective studies. Early diagnosis and patient education, progression monitoring, and timely surgical intervention remain the pillars of clinical management.
Nahata H, Nagaraja H, Shetty R. Topographic changes in contralateral eye of a case of Terrien’s marginal degeneration. BMJ Case Rep. 2022;15:e249493. doi:10.1136/bcr-2022-249493
Mandal S, Sachdeva G, Nagpal R, Maharana PK. Early onset unilateral Terrien’s marginal degeneration. BMJ Case Rep. 2022;15:e248889. doi:10.1136/bcr-2022-248889
Chan AT, Ulate R, Goldich Y, Rootman DS, Chan CC. Terrien Marginal Degeneration: Clinical Characteristics and Outcomes. American journal of ophthalmology. 2015;160(5):867-872.e1. doi:10.1016/j.ajo.2015.07.031. PMID:26210866.
Ding Y, Murri MS, Birdsong OC, et al. Terrien marginal degeneration. Surv Ophthalmol. 2019;64:162-174. doi:10.1016/j.survophthal.2018.09.004.
Vest A, Jean-Charles A, Bechet L, Plasse N, Paul N, Merle H.. [Terrien’s marginal corneal degeneration in a six-year-old girl: A case report]. J Fr Ophtalmol. 2018;41(9):e433-e435. doi:10.1016/j.jfo.2018.01.023. PMID:30391186.
Rodriguez M, Yesilirmak N, Chhadva P, Goldhagen B, Karp C, Galor A. High-Resolution Optical Coherence Tomography in the Differentiation of Inflammatory Versus Noninflammatory Peripheral Corneal Thinning. Cornea. 2017;36(1):48-52. doi:10.1097/ICO.0000000000001023. PMID:27631347; PMCID:PMC5138129.
Pouliquen Y, Renard G, Savoldelli M. Keratoconus associated with Terrien’s marginal degeneration. A clinical and ultrastructural study. Acta Ophthalmol Suppl. 1989;192:174-181. doi:10.1111/j.1755-3768.1989.tb07111.x.
Ruutila M, Fagerholm P, Lagali N, Hjortdal J, Bram T, Moilanen J, et al. Diagnostic Criteria for Terrien Marginal Degeneration: Nordic Terrien Degeneration Study. Cornea. 2021;40(2):133-141. doi:10.1097/ICO.0000000000002427. PMID:33155577.
Harada S, Mohamed YH, Kusano M, Inoue D, Uematsu M. Bilateral Fuchs’ Superficial Marginal Keratitis Diagnosis and Treatment. Life (Basel). 2024;14(12):1644. doi:10.3390/life14121644.
Farid M, Rhee MK, Akpek EK, Amescua G, Garcia-Ferrer FJ, Lin A, Varu DM, Musch DC, et al. Corneal Edema and Opacification Preferred Practice Pattern®. Ophthalmology. 2019;126(1):P216-P285. doi:10.1016/j.ophtha.2018.10.022. PMID:30366795.
Fernandes M, Vira D. Patch Graft for Corneal Perforation Following Trivial Trauma in Bilateral Terrien’s Marginal Degeneration. Middle East African journal of ophthalmology. 2015;22(2):255-7. doi:10.4103/0974-9233.151873. PMID:25949089; PMCID:PMC4411628.
Austin P, Brown SI. Inflammatory Terrien’s marginal corneal disease. American journal of ophthalmology. 1981;92(2):189-92. doi:10.1016/0002-9394(81)90768-6. PMID:7270631.
Chung J, Jin KH, Kang J, Kim TG. Spontaneous corneal perforation in Terrien’s marginal degeneration in childhood: A case report. Medicine. 2017;96(49):e9095. doi:10.1097/MD.0000000000009095. PMID:29245335; PMCID:PMC5728950.