
Corneal Dellen
Key Points at a Glance
Section titled “Key Points at a Glance”1. What is Corneal Dellen?
Section titled “1. What is Corneal Dellen?”Corneal dellen is a shallow, dish-shaped depression in the peripheral cornea adjacent to a paralimbal elevation. It was first described by Ernst Fuchs as a shallow, dish-shaped depression at the corneal margin.
It occurs due to localized disruption of the tear film, particularly deficiency of the mucin layer and dehydration 2). The tear film break causes localized corneal dehydration, leading to thinning of the stroma and formation of a depression. Limbal lesions and pterygium are the most common causes 2).
Usually resolves spontaneously within 24–48 hours, and most heal within 2 weeks. However, if chronic, it can lead to epithelial breakdown, stromal inflammation, and scarring.
In most cases, with appropriate lubrication such as artificial tears, it resolves within 24–48 hours. Most cases heal within 2 weeks, but if the causative elevation persists or treatment is delayed, it may become prolonged or worsen.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”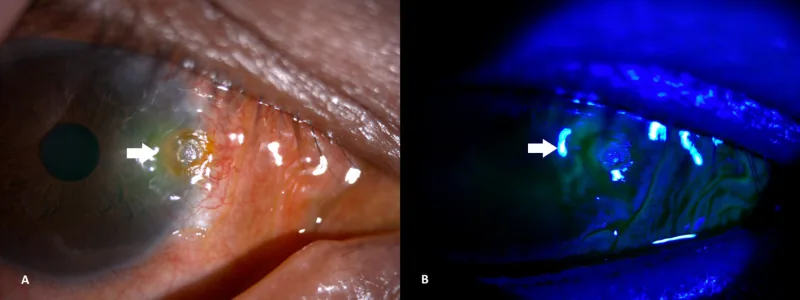
Subjective Symptoms
Section titled “Subjective Symptoms”Subjective symptoms of corneal dellen are relatively mild.
- Redness: Accompanied by dilation of adjacent conjunctival vessels.
- Foreign body sensation: Discomfort due to irregularity of the ocular surface
- Grittiness: Unpleasant sensation similar to dryness
Severe pain is rare, but if secondary infection occurs, pain, photophobia, and decreased vision may develop1).
Clinical Findings
Section titled “Clinical Findings”The following findings are observed on slit-lamp examination.
- Well-demarcated depression: A saucer-shaped depression occurs in the peripheral cornea, approximately 2–3 mm in diameter
- Predilection site: Usually occurs on the temporal side, presenting as an oval shape parallel to the limbus
- Wall morphology: The corneal side wall is steep, while the limbal side wall slopes gently
- Epithelial status: The epithelium covers the dehydrated, thinned stromal area. The epithelium may be transparent or appear opaque due to opacity and dryness
- Fluorescein findings: Fluorescein pools in the depression, and sometimes staining is observed at the top
- Corneal sensation: Sensation may be reduced in the dellen area compared to the surrounding area
- Adjacent changes: Vascular loops and conjunctival vessels are congested, but the adjacent cornea is usually normal
In a case secondary to subconjunctival silicone oil (SCSO), a dellen measuring 6×3 mm with infiltrate was observed at the 9 o’clock temporal position1). Anterior segment optical coherence tomography (AS-OCT) confirmed the depth of the dellen and the positional relationship between SCSO and subscleral silicone oil1).
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Corneal dellen are caused by local disruption of the tear film due to a limbal elevation. The main causes are listed below.
| Classification | Cause |
|---|---|
| Inflammatory | Episcleritis, scleritis |
| Degenerative/proliferative | Pinguecula, pterygium, limbal tumor |
| Postoperative | Glaucoma surgery, strabismus surgery, cataract surgery |
In addition to the above, the following causes are also known.
- Subconjunctival hemorrhage/conjunctival edema: Forms a bulge that disrupts the tear film
- Subconjunctival injection: Caused by a localized bulge from the medication
- Filtering bleb: A bleb after trabeculectomy bulges near the limbus
- Suture granuloma: Granulomatous reaction to postoperative sutures
- Subconjunctival silicone oil (SCSO): Silicone oil migrates under the conjunctiva after vitrectomy, forming a bulge. Migration under the conjunctiva has been reported in 9.7% of cases that underwent 23-gauge vitrectomy and silicone oil injection1)
- Long-term contact lens wear: Involves changes in tear film distribution
- Paralytic lagophthalmos: instability of the tear film due to incomplete eyelid closure
- Idiopathic: may be observed in elderly individuals
- Ocular trauma: conjunctival swelling or scarred elevation after injury
Occurrence after strabismus surgery and glaucoma filtration surgery has been reported2). Similar complications can also occur after glaucoma device (Ahmed valve) implantation2).
Corneal dellen can occur after glaucoma surgery (trabeculectomy, glaucoma device implantation), strabismus surgery, cataract surgery, and others2). Postoperative suture granulomas or filtering blebs may form a limbal elevation that disrupts the tear film.
4. Diagnosis and examination methods
Section titled “4. Diagnosis and examination methods”Medical history taking
Section titled “Medical history taking”Check the following history:
- History of eye surgery (glaucoma surgery, vitrectomy, strabismus surgery, etc.)
- Presence of ocular trauma
- Contact lens wear history
- Previous ocular symptoms
Examination Methods
Section titled “Examination Methods”- Slit-lamp microscopy: The basic finding is a well-defined depression in the peripheral cornea with an adjacent elevated lesion.
- Fluorescein staining: Confirms pooling of dye in the depression. If there is an epithelial defect, staining is observed.
- Anterior segment optical coherence tomography (AS-OCT): Objectively evaluates the depth of the dellen, the degree of thinning, and the positional relationship with the underlying subconjunctival lesion1).
Differential Diagnosis
Section titled “Differential Diagnosis”Corneal dellen is a non-inflammatory corneal thinning, and differentiation from the following diseases is important.
- Infectious corneal ulcer: Accompanied by infiltration and abscess, with clear staining of the epithelial defect. May have hypopyon.
- Catarrhal corneal ulcer: An immunogenic peripheral ulcer with localized ciliary injection.
- Mooren’s ulcer: A deeply excavated ulcer in the peripheral cornea, showing progressive tissue destruction.
- Terrien’s marginal degeneration: Slowly progressive peripheral corneal thinning, commonly occurring superiorly.
In dellen, the epithelium is usually intact and there is no infiltration, which is an important distinguishing point from corneal ulcers. However, secondary infection of dellen can lead to infiltration1).
5. Standard Treatment
Section titled “5. Standard Treatment”Elimination of the Cause
Section titled “Elimination of the Cause”The principle of treatment is to reduce the limbal elevation, i.e., to treat the underlying cause.
Conservative Treatment
Section titled “Conservative Treatment”The goal is to rapidly reconstruct the mucin layer and the hydrophilic corneal surface.
- Artificial tears and eye ointments: Frequent lubrication supplements the tear film and promotes corneal rehydration.
- Eye patching: Prevents evaporation and promotes tear retention.
- Bandage contact lens (BCL): A large-diameter soft contact lens protects the corneal surface and stabilizes the tear film.
In dellen secondary to a filtering bleb, the bleb cannot be removed because it is necessary for intraocular pressure control. Management involves long-term and frequent use of artificial tears.
Surgical Treatment
Section titled “Surgical Treatment”Surgical intervention is indicated when conservative treatment fails or when the causative elevation is clear.
- Excision of elevated lesions: Remove causative lesions such as pterygium, pinguecula, or limbal tumors.
- Tarsorrhaphy: May be performed to limit exposure of the ocular surface.
Management of Complications
Section titled “Management of Complications”In a case of dellen secondary to subconjunctival silicone oil complicated by infiltration, after resolving the infiltration with levofloxacin 1.5% eye drops (every hour) and gatifloxacin 0.3% eye ointment (at bedtime), surgical removal of subconjunctival SO, application of cyanoacrylate adhesive, and placement of a bandage contact lens were performed1).
Although rare, if dellen are left untreated, corneal stromal degeneration can progress and lead to perforation2). Additionally, secondary infection can cause serious complications such as perforation and endophthalmitis1). Early lubrication treatment and removal of the cause are important.
6. Pathophysiology and Detailed Mechanism
Section titled “6. Pathophysiology and Detailed Mechanism”The formation mechanism of corneal dellen involves the following steps:
- A perilimbal elevation locally disrupts the tear film.
- The mucin layer is absent at the site of tear film disruption.
- The corneal epithelium is normally hydrophobic and repels water in the absence of mucin.
- A dry spot (dellen) forms.
- Local dehydration progresses, causing thinning of the corneal stroma.
- A shallow saucer-shaped depression (dellen) is completed.
The limbus is a specialized region with dense vasculature, immune, and nervous systems, and contains corneal epithelial stem cells. Elevations near the limbus disrupt this delicate environment, leading to tear film instability.
Mahgoub et al. (2017) examined 20 eyes with subconjunctival silicone oil (SCSO) after 23-gauge vitrectomy and found dellen formation in 10 eyes (50%). Proximity of SCSO to the limbus was a risk factor for dellen development; the closer to the limbus, the higher the incidence. All dellen healed with scarring after SCSO removal 1).
Hyung & Min (1998) also reported resolution of dellen after removal of subconjunctival silicone oil leakage via a Molteno implant 1), indicating that removal of the causative elevation is key to healing.
Dellen are usually self-limiting, but if chronic, epithelial breakdown, stromal inflammation, and scarring may progress. Secondary infection of a dellen can lead to serious complications such as perforation or endophthalmitis 1). Early removal of the cause and restoration of the tear film are essential for preventing complications.
8. References
Section titled “8. References”
- Mohan S, Nadri G, Mohan S. A Rare Complication Causing Another Rare Complication: Corneal Dellen with Infiltration Secondary to Subconjunctival Silicon Oil. Beyoglu eye journal. 2023;8(3):233-236. doi:10.14744/bej.2023.74508. PMID:37766771; PMCID:PMC10521125.
- Marafon SB. Corneal Dellen. Arq Bras Oftalmol. 2024;87(3):e2023-0060.
- Sakallioğlu AK, Garip R. Corneal dellen development after strabismus surgery. Strabismus. 2021;29(4):221-227. PMID: 34719322.