Surgically induced necrotizing scleritis (SINS) is a rare complication in which inflammation and necrosis occur in the scleral tissue adjacent to the surgical wound after ophthalmic surgery. It most commonly occurs after multiple ophthalmic surgeries. Other terms for this condition include surgically-induced scleral necrosis and postoperative scleral melting.
The incidence is estimated to be less than 1 in 10,000 cases, with some reports suggesting less than 1 in 100,000 cases 2). Women account for approximately 70%, and the average age is 68.2 years 3). The average time from surgery to onset of SINS is 9 months, but it has been reported to range from a few days to up to 51 years postoperatively.
Among ophthalmic surgeries reported to be associated with SINS, pterygium surgery is the most common, accounting for 63.4% of cases. This is followed by cataract surgery at 17.5% and scleral buckling at 11.3% 3). Cases have also been reported after strabismus surgery, trabeculectomy, and vitrectomy. The risk is also increased with surgeries using mitomycin C.
QHow rare is SINS?
A
The incidence is less than 1 in 10,000 cases, with some estimates suggesting less than 1 in 100,000 cases 2). However, because the initial symptoms of SINS are mild, it may be overlooked, and the actual incidence may be higher. It has been pointed out that scleral necrosis after pterygium surgery may not be correctly diagnosed as SINS 4).
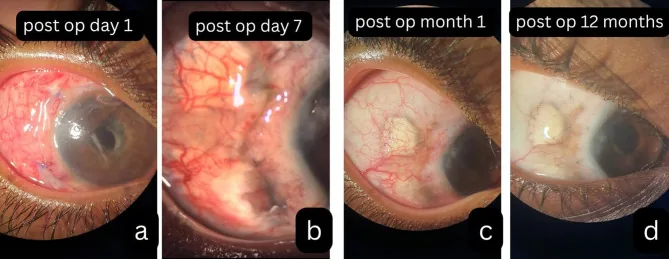
Kohli GM, Singh L, Masood A, et al. Multifocal necrotising scleritis post-MIVS in oligoarticular JIA : exploring plausible deniability. Journal of Ophthalmic Inflammation and Infection. 2025 Dec 6; 16:1. Figure 2. PMCID: PMC12796035. License: CC BY.
Anterior segment photographs from the early postoperative period to long-term follow-up are shown, illustrating the progression of scleral necrosis and scarring near the surgical wound. The sequence demonstrates worsening tissue loss and vascular changes as inflammation progresses.
Scleral necrosis adjacent to the surgical wound: Inflammation and necrosis of the scleral tissue adjacent to the surgical site are characteristic. The sclera becomes thin and takes on a “porcelainized” appearance 3).
Uveal show and prolapse: In severe necrosis, the uvea may be visible through the thinned sclera. Perforation may occur.
Complication of necrotizing keratitis: Inflammation may spread to the cornea, sometimes accompanied by peripheral corneal infiltration 3).
Spread to posterior scleritis: Rarely, inflammation spreads posteriorly, causing posterior scleritis. Cases of diffuse anterior scleritis after pterygium surgery complicated by posterior scleritis have been reported 4).
Intraocular inflammation: Inflammatory cells in the anterior chamber and keratic precipitates may appear 1).
Nakagawa et al. reported a case of SINS complicated by Stenotrophomonas maltophilia infection after scleral buckling surgery. After buckle removal, scleral thinning and intraocular inflammation progressed, and corrected visual acuity decreased from 20/25 to 20/1000, but recovered to 20/32 after initiation of oral steroids 1).
The exact pathophysiology of SINS is unknown. A delayed-type hypersensitivity reaction (type IV allergic reaction) to degenerated or exposed scleral tissue antigens caused by surgery is considered the main mechanism. Pathological studies have shown IgM and IgG deposition, increased HLA-DR expression, and involvement of helper T cells in conjunctival biopsies.
There is a strong association between SINS and systemic autoimmune diseases. Many cases of underlying systemic disease are discovered during workup after the onset of SINS. About half of SINS cases after cataract surgery have a history of systemic disease, with rheumatoid arthritis being the most common 3).
Diabetes mellitus: Promotes an ischemic and inflammatory environment 2). In diabetic patients, attention should also be paid to co-infection with opportunistic infections such as tuberculosis 3).
Female sex: Approximately 70% of patients are female 3).
QWhy does mitomycin C increase the risk of SINS?
A
Mitomycin C (MMC) is an antimetabolite that suppresses fibroblast proliferation and delays scleral wound healing. Its adjunctive use in pterygium surgery and trabeculectomy induces local ischemia and leads to scleral weakening. It has been reported that 82% of SINS cases after pterygium surgery were associated with the use of mitomycin C or beta irradiation. However, since normal sclera has almost no blood vessels, ischemia alone cannot explain the entire process, and involvement of immunological mechanisms is also suspected.
History and examination: SINS is a clinical diagnosis based on a history of eye surgery and the presence of necrotizing scleritis adjacent to the surgical wound.
Exclusion of infection: Bacterial culture, PCR testing, and scleral biopsy are used to rule out infectious causes 2). PCR analysis of conjunctival scrapings and aqueous humor is recommended.
Systemic Examination
Autoimmune screening: Evaluate RF, ANA, ANCA (PR3-ANCA, MPO-ANCA), CRP, and HLA-B27 2).
Infectious disease screening: Perform tuberculin skin test, IGRA (interferon-gamma release assay), and chest X-ray 3). Exclusion of tuberculosis is especially important in tuberculosis-endemic areas.
In infectious scleritis, Pseudomonas aeruginosa is the most common, accounting for up to 85% of cases. Other organisms include Staphylococcus aureus and Streptococcus pneumoniae. Fungal scleritis is the most severe and difficult to control due to poor penetration of antifungal agents.
Autoimmune necrotizing scleritis is clinically similar to SINS, but it is often bilateral and not necessarily associated with a history of ocular surgery. If there is a history of multiple ocular surgeries and scleritis occurs at the surgical site, a diagnosis of SINS is preferred.
SINS may also be complicated by infection. It has been reported that infection was involved in 97.2% of SINS cases after scleral buckling surgery 3). Infection was also associated with 71.4% of SINS cases after pterygium surgery 3).
QHow is SINS differentiated from infectious scleritis?
A
Infectious scleritis is diagnosed by identifying the pathogen through culture or PCR. SINS is diagnosed after excluding infection, based on a history of surgery and the presence of necrotizing scleritis adjacent to the surgical wound. However, co-occurrence is common, especially after scleral buckling surgery (97.2%) and pterygium surgery (71.4%), where concurrent infection and SINS have been reported 3). If there is no improvement with antibiotic therapy for infection, consider the possibility of concurrent SINS and evaluate steroid therapy 1).
Before starting treatment for SINS, it is extremely important to rule out an infectious cause.
First-line: High-dose oral prednisolone is the standard treatment for acute SINS. Topical prednisolone eye drops may also be used concomitantly. NSAIDs are not recommended as first-line therapy for SINS.
Severe cases: Intravenous methylprednisolone pulse therapy (1,000 mg/day for 3 days) is administered.
Refractory cases: Switch to immunosuppressive agents such as azathioprine or cyclophosphamide. Biologics (infliximab, rituximab) have also been reported to be effective.
Cases with concurrent infection: Administer steroids in parallel with antibiotic therapy. If SINS inflammation persists even after infection is controlled, systemic steroid administration is essential 1).
Cases with concurrent tuberculosis: Initiate anti-tuberculosis therapy (isoniazid, rifampicin, pyrazinamide, ethambutol). Ruiz-Lozano et al. reported that scleral necrosis resolved one month after starting anti-tuberculosis therapy in a case of SINS with tuberculosis that developed 12 years after pterygium surgery 3).
In the report by Nakagawa et al., oral administration of methylprednisolone 30 mg/day for SINS after scleral buckling surgery resulted in resolution of intraocular inflammation and coverage of the thinned sclera with conjunctival tissue. Corrected visual acuity improved from 20/1000 to 20/32, and remained stable for 2 years with a low dose (1 mg/day) 1).
The timing of treatment initiation greatly affects visual prognosis. It has been reported that patients who started high-dose steroids within 1 month of onset had an average decrease of only 1 to 3 lines on the Snellen visual acuity chart, whereas those who started treatment after 3 months showed a permanent visual loss of 5 lines or more. To avoid structural destruction due to scleral staphyloma or scleral melting, it is important to start systemic steroid therapy promptly after ruling out infection.
The underlying mechanism of SINS is thought to be a type IV hypersensitivity reaction (delayed-type hypersensitivity) to tissue antigens such as scleral collagen exposed by surgery. Surgical trauma triggers the deposition of immune complexes on scleral vessel walls. Pathologically, deposition of IgM and IgG, increased HLA-DR expression, and infiltration of T helper cells have been confirmed.
SINS is thought to manifest pre-existing subclinical autoimmune diseases. In cases with a latency period of several years or more from surgery to onset of SINS, it is likely that a systemically induced immune reaction later spread to the eye. In about half of SINS cases after cataract surgery, systemic autoimmune diseases (especially rheumatoid arthritis) are found 3).
Mitomycin C and beta irradiation induce local vascular damage and ischemia. However, since normal sclera is inherently poorly vascularized, ischemia alone cannot explain the entire process of necrosis. Enzymatic degradation of scleral collagen due to surgical manipulation and epithelial disruption has been proposed as the main mechanism. In patients with connective tissue disease, collagenase-related vasculitis affecting the deep episcleral venous plexus is also involved.
Infection can be interpreted as either a direct cause of SINS or a secondary complication. Postoperative vascular damage, tissue destruction, and delayed wound healing create a substrate for infection 3). After scleral buckling surgery, the infection rate is particularly high at 97.2% 3). On the other hand, it has also been suggested that infection may amplify the immune response in SINS.
Matsuura et al. reported a case of SINS that developed 18 months after pterygium excision (conjunctival autograft combined with mitomycin C). In this case, diffuse anterior scleritis was accompanied by posterior scleritis, which is the first report of posterior scleritis after pterygium surgery. Numerous granulomatous deposits were observed on the iris surface, but infection and malignancy were ruled out, and intraocular inflammation due to immunological mechanisms was concluded 4).
Nakagawa Y, Suzuki T, Suzuki Y. Surgically-Induced Necrotizing Scleritis After Scleral Buckling With Stenotrophomonas maltophilia Infection. Cureus. 2024;16(2):e53876. doi:10.7759/cureus.53876.
Vatkar V, Bhavsar D, Agrawal T, Potdar PP, Jakhalu K. Necrotizing Scleritis Post Cataract Surgery: A Diagnostic Dilemma. Cureus. 2024;16(10):e70861. doi:10.7759/cureus.70861. PMID:39493025; PMCID:PMC11531864.
Ruiz-Lozano RE, Rodriguez-Garcia A, Colorado-Zavala MF, Alvarez-Guzman C. Surgically induced scleral necrosis associated with concomitant tuberculosis infection: a diagnostic challenge. GMS ophthalmology cases. 2023;13:Doc04. doi:10.3205/oc000212. PMID:36875627; PMCID:PMC9979078.
Matsuura K, Terasaka Y. Diffuse anterior and posterior scleritis with multiple iris granular deposits following pterygium excision. Romanian journal of ophthalmology. 2021;65(4):399-402. doi:10.22336/rjo.2021.79. PMID:35087985; PMCID:PMC8764424.
Ruiz-Lozano RE, Garza-Garza LA, Davila-Cavazos O, Foster CS, Rodriguez-Garcia A. The clinical and pathogenic spectrum of surgically-induced scleral necrosis: A review. Survey of ophthalmology. 2021;66(4):594-611. doi:10.1016/j.survophthal.2020.12.008. PMID:33422510.
Akbari MR, Mohebbi M, Johari M, Mirmohammadsadeghi A, Mahmoudi A. Multifocal Surgically Induced Necrotizing Scleritis Following Strabismus Surgery: A Case Report. Strabismus. 2016;24(3):101-5. doi:10.1080/09273972.2016.1205104. PMID:27485819.
O’Donoghue E, Lightman S, Tuft S, Watson P. Surgically induced necrotising sclerokeratitis (SINS)—precipitating factors and response to treatment. Br J Ophthalmol. 1992;76(1):17-21. doi:10.1136/bjo.76.1.17. PMID:1739684; PMCID:PMC504142.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.