Keratoglobus is a rare non-inflammatory corneal ectasia in which the entire cornea becomes diffusely thinned and protrudes forward in a spherical shape. The corneal diameter is normal, but the cornea is thin, often accompanied by scleral thinning. It is a rare disease, usually congenital and seen in children 5).
It presents with high myopia and irregular astigmatism, often difficult to correct with spectacles or contact lenses 4). Corneal rupture can occur from external force.
QWhat is the difference from keratoconus?
A
Keratoconus is characterized by localized thinning and protrusion in the central to inferior cornea. In contrast, keratoglobus involves diffuse thinning and spherical protrusion of the entire cornea. Fleischer rings and Vogt striae are seen in keratoconus but are not typical in keratoglobus. Keratoconus usually develops after age 10, while the congenital form of keratoglobus is present at birth. Eye rubbing is a risk factor for keratoconus but not specified for keratoglobus.
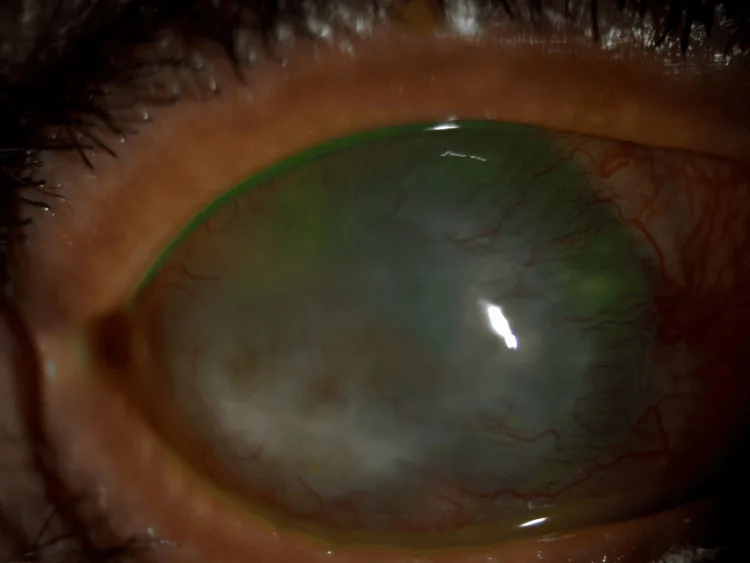
Yumna F Kamal, Mazen Alzahrani, Halah Bin Helayel, Sami T Hameed Trypan Blue and Endoillumination-Assisted Phacoemulsification in a Patient With Advanced Keratoglobus 2024 Mar 16 Cureus.; 16(3):e56265 Figure 1. PMCID: PMC11017366. License: CC BY.
Medical image of keratoglobus showing a diffusely thin, protruding cornea with extensive opacity.
Visual loss is due to high myopia and irregular astigmatism. Often, adequate correction cannot be achieved with glasses or contact lenses 3). Acute hydrops or spontaneous rupture of Descemet’s membrane may be accompanied by severe eye pain.
Corneal globular protrusion: The entire cornea protrudes forward in a spherical shape. It is prominent when observed from the side.
Diffuse thinning: Most pronounced in the peripheral cornea. Peripheral corneal thickness can thin to 330 μm or less 1).
Descemet’s membrane abnormalities: Folds, breaks, and thickening are often observed. Spontaneous rupture of Descemet’s membrane can cause acute hydrops.
Increased anterior chamber depth: May present with a deep anterior chamber exceeding 5 mm 1).
Findings Useful for Differential Diagnosis
Fleischer ring and Vogt striae: Typically not present in keratoglobus. These are characteristic findings of keratoconus.
Corneal curvature: May reach 50–60 D. The entire cornea becomes steeper compared to keratoconus.
Scleral thinning: Often accompanied by scleral thinning, which may present as blue sclera.
The etiology is unknown, but it is thought to be related to defects in collagen synthesis or degradation. Associations with Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta, and blue sclera syndrome suggest that collagen abnormalities may be the cause.
In keratectasia, an increase in matrix metalloproteinases (MMPs) and a decrease in their inhibitors (TIMPs) have been reported 5). These enzymes may be involved in the degradation of the corneal stroma5).
Unlike keratoconus, eye rubbing is not recognized as a risk factor. An association with atopic diseases has also not been identified.
Ehlers-Danlos syndrome is a group of disorders characterized by connective tissue fragility due to abnormalities in collagen structural genes. It features skin hyperextensibility, joint hypermobility, and ocular fragility, with a high risk of globe rupture. In Down syndrome, the risk of keratectasia is reported to be about 100 times higher 4).
Clinical diagnosis is made by slit-lamp microscopy. Essential findings include globular protrusion of the cornea and diffuse thinning that is most pronounced in the periphery.
AS-OCT provides high-resolution cross-sectional images of the cornea, anterior chamber, and angle 5). Pachymetry mapping can quantitatively evaluate the distribution of thinning 5).
In keratoconus, localized thinning and protrusion are observed in the central to inferior cornea. Pellucid marginal degeneration shows a band-like thinning of the inferior peripheral cornea while remaining transparent. Keratoglobus is differentiated by its onset at birth in both eyes and thinning of the entire cornea.
Management begins with spectacle correction. Polycarbonate lenses deform rather than shatter, making them useful for corneal protection as well. The safety of contact lenses is debated. Fitting of RGP lenses must be performed carefully.
No gold standard has been established for surgical treatment of keratoglobus 1).
Corneal Transplantation
Conventional PK: Technically less difficult, but because a normal-thickness graft is joined to a very thin recipient tissue, high postoperative astigmatism is likely to occur1).
Femtosecond laser-assisted half top hat PK: A top hat configuration is created only in the donor cornea. The configuration with an outer diameter of 9.5 mm and a central full-thickness button of 7.1 mm increases peripheral corneal thickness1). Two cases have been reported in which best-corrected visual acuity (BCVA) improved to 20/30–20/401).
Lamellar keratoplasty: Provides structural support and preserves limbal stem cells5). In cases of diffuse thinning, it may flatten the cornea, but significant folds can occur5).
Two-stage surgery: A method in which PK is performed 6 months after lamellar transplantation, indicated when corneal opacity remains.
Special Surgical Cases
Sclerokeratoplasty (SKP): Useful for anterior segment reconstruction in cases of extensive corneal rupture2). Because a large graft extending beyond the limbus is used, strong suturing is possible2). However, the rejection rate is high, approximately 70%2).
Simultaneous SKP and vitrectomy: There is a report of performing 25G vitrectomy after SKP for a globular cornea complicated by corneal rupture and intraocular hemorrhage2). Fundus visibility through the graft was good2).
Modified phacoemulsification: For advanced globular cornea with cataract, a technique using a scleral flap approach with trypan blue staining and endoscopic illumination has been reported3). It is useful for improving visibility under corneal opacity3).
QIs surgery always necessary?
A
In mild globular cornea, management with glasses or contact lenses may be sufficient. Surgery is indicated when conservative treatment does not provide adequate vision, when there is corneal opacity or scarring, or when corneal rupture recurs. Because surgery carries risks such as graft rejection, high astigmatism, and epithelial healing failure, the indication should be carefully considered.
QWhat is the prognosis after corneal transplantation?
A
The prognosis after corneal transplantation varies depending on the surgical technique and the case. In femtosecond laser-assisted half top hat PK, it has been reported that best corrected visual acuity improved to 20/30–20/40 in two cases, with no rejection or complications during 12–24 months of follow-up 1). On the other hand, SKP has a high rejection rate of approximately 70% 2), requiring long-term immunosuppression. Overall, the surgical prognosis for keratoglobus is poor and is associated with many complications.
Histological features of keratoglobus include diffuse corneal stromal thinning and focal breaks in Bowman’s layer, most prominent in the periphery. Despite thinning, the lamellar structure of the stroma remains unchanged from its normal configuration. Other findings include central epithelial hyperplasia, stromal neovascularization and scarring, and breaks and thickening of Descemet’s membrane.
In non-inflammatory corneal ectasia, decreased α1-proteinase inhibitor (α1-PI) and increased transcription factor Sp1 in the corneal stroma have been reported. Similar changes are observed in keratoglobus, and alterations in stromal degradation processes are thought to be the underlying cause of corneal thinning.
In corneal ectasia in general, increased matrix metalloproteinases (MMPs) and decreased TIMPs have been reported 5). An imbalance of these enzymes may contribute to corneal stromal degradation 5). Elevated tear levels of inflammatory mediators (IL-6, TNF-α, MMP-9) have also been reported, which may induce corneal cell apoptosis5). This suggests that inflammatory components may be involved even in corneal ectasia classified as non-inflammatory 5).
Keratoglobus differs from keratoconus in that it is not associated with atopic diseases. It is presumed that a defect in collagen synthesis or degradation underlies the condition.
Femtosecond laser-assisted half top hat PK is a relatively new technique that creates a top hat configuration only in the donor cornea1). In conventional top hat PK, both donor and recipient are shaped, but this method avoids manipulation of the extremely thin recipient cornea1). In a report of two cases, best corrected visual acuity improved to 20/30, with increased peripheral corneal thickness and structural stability 1). Future challenges include size customization based on the patient’s corneal diameter and verification of long-term outcomes 1).
Simultaneous SKP and 25-gauge vitrectomy for keratoglobus complicated by corneal rupture and intraocular hemorrhage has been reported 2). Advances in wide-angle viewing systems and chandelier illumination have improved fundus visibility through the graft after corneal transplantation, enabling vitrectomy without the use of artificial corneas or endoscopes 2).
Femtosecond laser-assisted half top hat PK is a relatively simple procedure that provides good anatomical and visual outcomes. In the future, simultaneous cataract surgery and accumulation of long-term postoperative results are needed. 1)
Corneal cross-linking has been reported in a pediatric case (6-month-old infant) with keratoglobus associated with Down syndrome4). The efficacy of cross-linking for keratoglobus requires further investigation.
Palevski D, Marom NR, Livny E, Nahum Y, Levinger S, Bahar I. Femtosecond laser-assisted half top hat penetrating keratoplasty for keratoglobus. American journal of ophthalmology case reports. 2025;39:102406. doi:10.1016/j.ajoc.2025.102406. PMID:40791656; PMCID:PMC12337701.
Higashijima F, Aoki R, Mikuni M, Yoshimoto T, Iwamoto N, Ohta M, et al. Simultaneous Vitreoretinal Surgery and Sclerokeratoplasty for Keratoglobus with Intraocular Hemorrhage and Extensive Corneal Rupture. Case reports in ophthalmology. 2022;13(1):220-226. doi:10.1159/000522282. PMID:35611013; PMCID:PMC9082195.
Kamal YF, Alzahrani M, Bin Helayel H, Hameed ST. Trypan Blue and Endoillumination-Assisted Phacoemulsification in a Patient With Advanced Keratoglobus. Cureus. 2024;16(3):e56265. doi:10.7759/cureus.56265.
Bjelos M, Ćurić A, Busić M, Rak B, Kuzmanović Elabjer B, Marković L. Novel Variant IMPDH1 c.134A>G, p.(Tyr45Cys): Phenotype-Genotype Correlation Revealed Likely Benign Clinical Significance. Int J Mol Sci. 2023;24(15):11889. doi:10.3390/ijms241511889. PMID:37569264; PMCID:PMC10419040.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.