Syphilitic interstitial keratitis is a non-ulcerative corneal stromal inflammation caused by Treponema pallidum infection, accounting for approximately 90% of clinically recognized interstitial keratitis. It can occur in both congenital and acquired syphilis, but is overwhelmingly more common in congenital syphilis.
Worldwide, 5.7 to 6 million new cases of syphilis are reported annually 1). In Japan, the number has increased markedly since 2011, with fewer than 1,000 cases reported in 2011 but exceeding 6,000 in 2017. Since the development of penicillin, the incidence of syphilitic keratitis has decreased dramatically, but it has not been eradicated.
Congenital syphilis occurs via transplacental infection and is classified by onset into fetal syphilis, early congenital syphilis (up to 2 years), and late congenital syphilis (after 2 years to adolescence). The findings of late congenital syphilis are known as Hutchinson’s triad (Hutchinson teeth, interstitial keratitis, and sensorineural hearing loss). It is usually bilateral and more common in females.
In acquired syphilis, ocular symptoms occur with systemic symptoms from the secondary stage onward. In the United States, surveillance from 2014 to 2015 found ocular symptoms in 0.6% of syphilis patients. Interstitial keratitis in acquired syphilis shows similar pathology to congenital syphilis but tends to be unilateral and has less corneal neovascularization.
QWhat is Hutchinson's triad?
A
It is a combination of three findings characteristic of late congenital syphilis: Hutchinson teeth (notched incisors of the upper jaw), interstitial keratitis, and sensorineural hearing loss1). Interstitial keratitis typically develops from school age to adolescence and is usually bilateral. In Japan, due to improved perinatal care, new cases of late congenital syphilis have become extremely rare.
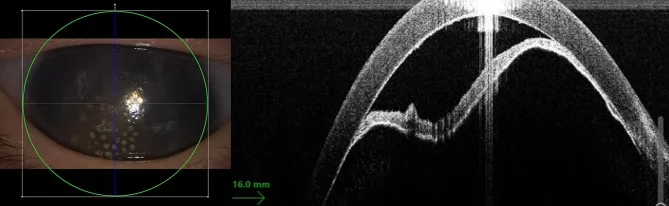
Haecke HV, Roels D, Nerinckx F, et al. Spiroplasma infection as a cause of severe congenital keratouveitis, cataract and glaucoma. BMC Ophthalmology. 2024 May 21; 24:217. Figure 2. PMCID: PMC11106900. License: CC BY.
An anterior segment photograph and anterior segment OCT are shown side by side, illustrating stromal opacity and cross-sectional changes of the cornea. The deep lesions seen in syphilitic keratitis can be appreciated both clinically and tomographically.
Photophobia: Occurs with the spread of inflammation to the corneal stroma.
Lacrimation: Often complicated by anterior uveitis, which intensifies symptoms1).
Decreased visual acuity: Occurs with progression of corneal opacity. If corneal opacity persists during the scarring stage, decreased visual acuity continues.
Clinical Findings (Findings Confirmed by Physician Examination)
Corneal stromal inflammation: Severe ciliary injection and diffuse or multifocal corneal cellular infiltration are observed. The deep corneal stroma is primarily affected, often starting from the superior region.
Salmon patch: A salmon-colored patch formed by a combination of corneal neovascularization and lymphatic dilation. This is a characteristic finding in the active stage.
Ghost vessels: In the scarring stage, vascular lumens with interrupted blood flow remain in the deep corneal stroma. Some are patent and may carry red blood cells.
Retrocorneal hyaline ridge (glass ridge): A needle-like structure observed on the endothelial surface, characteristic of the scarring stage.
Anterior uveitis: Complicated by iritis, with possible mutton-fat keratic precipitates and posterior synechiae.
When inflammation is severe, the basic structure of the cornea may break down, leading to endothelial damage and loss of Descemet’s membrane.
The causative microorganism is Treponema pallidum. However, this disease is thought to result from an immune reaction to treponemal antigens rather than direct infection by T. pallidum itself. The fact that corneal lesions are resistant to systemic penicillin but respond to steroids supports this hypothesis1).
Congenital syphilis: The risk of infection to the infant increases if the mother does not receive treatment before the second trimester of pregnancy1).
HIV co-infection: Co-infection with syphilis is increasing, raising the risk of ocular syphilis.
MSM (men who have sex with men): One of the main populations contributing to the recent increase in syphilis 1).
Slit-lamp microscopy: If bilateral keratitis with deep corneal vascular invasion is observed, consider syphilitic interstitial keratitis. Check for ghost vessels and glass ridges.
Indirect illumination: Useful for observing deep corneal neovascularization. Scleral scatter method clearly visualizes the extent of scar opacity.
Serological Tests
STS (RPR): Measures antibodies using lipid antigens. Highly sensitive and becomes positive early, but also has many biological false positives. RPR ≥16-fold indicates high activity.
TP antigen test (TPHA): Uses Treponema pallidum antigens and has excellent specificity. Essential for definitive diagnosis, but remains positive after treatment, so not suitable for treatment evaluation. TPHA ≥1,280-fold indicates high activity.
In latent syphilis and syphilitic keratitis, non-treponemal antibody titers may be low, so it has been suggested to start with treponemal testing 1).
Differential diagnoses for interstitial keratitis include tuberculosis, herpes simplex, and herpes zoster. Comprehensive evaluation of history, course, and serological findings is important. For diagnosis of syphilitic uveitis, syphilitic psoriasis and syphilitic roseola on the palms can also aid diagnosis.
Oral synthetic penicillin is used for systemic treatment of syphilis. In cases complicated by congenital syphilis or neurosyphilis, intravenous infusion of benzylpenicillin potassium or ceftriaxone is administered. The CDC guidelines recommend that any manifestation of ocular syphilis be treated according to neurosyphilis protocols (penicillin G for 14 days) 1).
The effect of antisyphilitic therapy is assessed by the change in RPR titer, with a target of a titer of 8-fold or less, or a decrease to 1/4 of the initial value.
The first-line treatment for syphilitic keratitis is steroid eye drops. Corneal lesions are resistant to penicillin but respond well to steroids 1). In cases with severe inflammation, steroid eye drops are used concurrently with antisyphilitic therapy.
Because long-term use of steroid eye drops carries risks of cataracts and glaucoma, cyclosporine or tacrolimus is recommended for recurrent syphilitic keratitis. There are reports that immunosuppressants are superior to steroids in preventing recurrence.
In cases of severe corneal opacity, penetrating keratoplasty (PKP) is indicated. The 10-year graft survival rate is reported to be approximately 80%. In cases where normal vision is not achieved, amblyopia due to childhood syphilitic keratitis is suspected.
QWhy does keratitis not heal with antibiotics?
A
The pathogenesis of syphilitic keratitis is not direct infection by T. pallidum but an immune reaction to treponemal antigens. Spirochetes are not detected in the cornea, and it does not respond to antibiotics but responds well to steroids. This supports an immune-mediated pathogenesis 1). However, systemic antisyphilitic therapy is necessary for systemic syphilis infection and is performed separately from local corneal treatment.
Experimental studies have shown that T. pallidum can adhere to corneal stromal cells and enter the eye hematogenously, but it is difficult to detect spirochetes in eyes affected by syphilitic keratitis 1). Therefore, it is thought that the pathogenesis is centered on an immune reaction rather than direct corneal infection.
A leading hypothesis is that immune-mediated inflammation is triggered by a delayed-type hypersensitivity reaction to residual treponemal antigens in the cornea, or by molecular mimicry with self-antigens 1). Histopathologically, lymphocytic infiltration and vascular invasion are observed in the corneal stroma.
Following bilateral iritis lasting several weeks, intense ciliary injection and diffuse corneal cellular infiltration occur. Subsequently, scarring deep corneal opacification with vascular invasion develops. The condition subsides within 3 to 6 months after onset, leaving ghost vessels as empty vascular lumens. The opacification gradually tends to resolve but often does not completely disappear.
Even after appropriate treatment, recurrence occurs in 5–15% of patients.
QWhat are ghost vessels?
A
Ghost vessels are vascular remnants without blood flow observed in the scarring stage of syphilitic interstitial keratitis. New blood vessels that invaded the corneal stroma during the active phase lose blood flow after inflammation subsides and remain as empty tubular structures. They are found in the deep corneal stroma and are an important sign of a history of syphilitic interstitial keratitis. Some ghost vessels remain patent and may carry red blood cells.
Chauhan K, Tyagi M, Naik M, et al. Demystifying Ocular Syphilis: A Major Review. Ocul Immunol Inflamm. 2023. DOI:10.1080/09273948.2023.2217246.
Dixon J. Recurrent Syphilitic Keratitis. Br Med J. 1873 Mar 1;1(635):223. PMID: 20746987.
Weisenberg de Gerber M, Dragone de Lewis R, Alberti de Cortés AM, Manera OO. [Syphilitic keratitis]. Rev Fac Cienc Med Cordoba. 1969;27(1):27-35. PMID: 5379763.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.