The cornea is normally avascular. Avascularity is maintained by a balance between angiogenic and anti-angiogenic factors. When this balance is disrupted, corneal neovascularization occurs. Fat components accumulate adjacent to new vessels, causing lipid keratopathy. This leads to corneal opacity, irregular astigmatism, and vision loss.
The principle of MICE is derived from transarterial chemoembolization (TACE) for hepatocellular carcinoma. In TACE, anticancer drugs are injected into the tumor’s arterial system to induce local tumor necrosis. MICE applies this principle by selectively injecting MMC into corneal neovessels. The irreversible cytotoxicity of MMC to vascular endothelial cells induces occlusion and regression of abnormal vessels 1).
QHow is MICE different from conventional corneal neovascularization treatments?
A
Conventional treatments (steroid eye drops, anti-VEGF therapy, laser photocoagulation) show some efficacy for acute corneal neovascularization but have limited effect in regressing mature vessels or chronic corneal neovascularization1). The major difference is that MICE utilizes the irreversible cytotoxicity of MMC to the vascular endothelium, so a direct occlusive effect can be expected even for mature vessels.
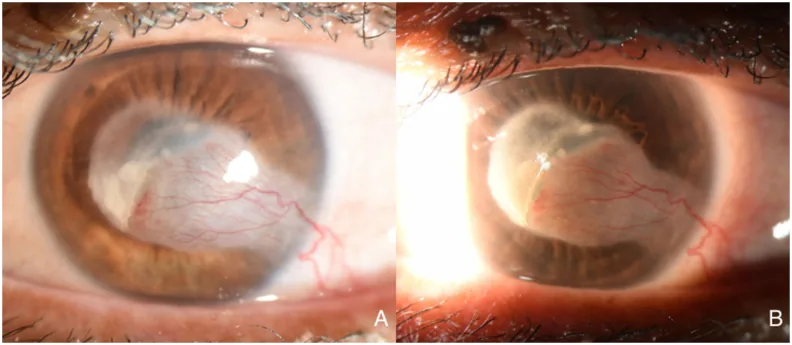
Neal Rangu, Kamran M Riaz Mitomycin intravascular chemoembolization (MICE) to treat corneal vascularization prior to penetrating keratoplasty 2024 Jan 14 Am J Ophthalmol Case Rep. 2024 Jan 14; 33:101993 Figure 3. PMCID: PMC10828578. License: CC BY.
A and B both show new blood vessels extending from the periphery to the center of the cornea, with surrounding white lipid deposits. In B, scleral scatter illumination more clearly reveals the extent of lipid deposition and opacity near the visual axis.
Corneal neovascularization: Blood vessels invade the corneal stroma superficially or deeply. Identification of feeder vessels is important for treatment planning.
Lipid keratopathy: White-yellow lipid deposits adjacent to new blood vessels, more likely when deep vessels are present. “Wet” lipid keratopathy presents with dense deposits that block light transmission 1).
Corneal stromal scarring: Results from chronic inflammation associated with neovascularization.
Ghost vessels: Observed as inactive vessels with no blood flow.
A characteristic finding after MICE is a “pizza-pie cornea” appearance in the early postoperative period 1). This is due to residual lipid and blood in the corneal stroma, which are reabsorbed over several weeks 1).
Deep neovascularization occurs when new vessels from the anterior ciliary arteries invade the corneal stroma, driven by persistent inflammation and stromal edema. Superficial neovascularization is associated with corneal epithelial hypoxia and conjunctival epithelial invasion.
Lipid keratopathy occurs secondary to corneal neovascularization. White opacities (lipid deposits) accumulate along the course of new vessels and gradually expand. This is more likely when deep neovascularization is present.
Preoperative confirmation of vascular morphology is essential. Identification of large vessels that are easy to cannulate is key to procedural success. The location and course of feeder vessels should be evaluated in detail using a slit lamp microscope.
Use as a prophylactic treatment before corneal transplantation has also been reported 1). Eyes with corneal neovascularization have a significantly higher rate of corneal graft rejection1). By removing central neovascularization with MICE, improved transplant success rates are expected 1).
The procedure is performed under an ophthalmic surgical microscope.
Topical anesthesia is applied to the operative eye, and preoperative disinfection is performed
A 1.0 cc tuberculin syringe is filled with MMC (0.4 mg/mL) and fitted with a 33-34 gauge TSK needle
The thickest corneal vessel is identified inside the limbus
The needle is inserted at an angle of approximately 15 degrees from the corneal surface. The bevel of the needle is positioned entirely within the corneal stroma
A small amount of MMC (0.01–0.05 mL) is injected. Hydrostatic pressure allows MMC to reach both afferent and efferent vessels
Confirm blanching of the blood vessels
Irrigate the ocular surface thoroughly with saline solution
Key Points of the Procedure
Needle gauge: Use 33-34 gauge. Needles thicker than 32 gauge are not recommended
Injection direction: Inject away from the corneal limbus to avoid damaging the limbal vascular network
Confirmation of blanching: If the blood vessels do not blanch, it may indicate intrastromal injection
Thorough irrigation: Since MMC is toxic to the corneal epithelium, thorough irrigation of the ocular surface is essential
Points to Note
Avoid full-thickness perforation: Full-thickness corneal perforation risks injecting MMC into the anterior chamber
Effect on corneal endothelium: The effect of MMC on corneal endothelial cells is unknown1)
Postoperative management: Use antibacterial and steroid eye drops after surgery
Steroid eye drops: Most effective when started in the acute phase, but have little effect on regression of mature vessels1)
Anti-VEGF therapy: Bevacizumab etc. are used, but are only effective for early corneal neovascularization and target only VEGF-A1). The presence of pericytes reduces efficacy1)
Laser photocoagulation: Identification of feeder vessels is difficult, and recurrence due to VEGF upregulation is observed1)
Fine-needle diathermy (FND): Good results have been reported when combined with bevacizumab1)
Occlusion of corneal neovascularization can be confirmed early after surgery (including on postoperative day 1)1). Residual lipid and blood in the corneal stroma are observed for several weeks after surgery but are reabsorbed1). As lipids are absorbed, corneal flattening occurs, causing transient astigmatism, which stabilizes or improves.
If residual vessels are present, MICE can be repeated. In successfully embolized vessels, no recurrence has been reported within the limited follow-up period.
Corneal transparency depends on avascularity. Avascularity is actively maintained by a balance between pro-angiogenic factors (e.g., VEGF) and anti-angiogenic factors1). When this balance is disrupted by infection, trauma, hypoxia, etc., corneal neovascularization occurs.
Superficial neovascularization involves invasion from conjunctival vessels into the subepithelial cornea. It is mainly caused by oxygen deficiency or conjunctival epithelial invasion. Deep neovascularization involves invasion from anterior ciliary arteries into the corneal stroma and occurs with persistent inflammation or stromal edema.
The vessel walls of corneal neovascularization have increased permeability compared to normal limbal vessels. Due to this increased vascular permeability, lipids in plasma components leak and deposit in the corneal stroma around the vessels. They spread as white opacities along the course of the new vessels.
MMC is an antitumor antibiotic derived from Streptomyces caespitosus. It has a cell proliferation inhibitory effect through DNA cross-linking. It shows irreversible cytotoxicity particularly to vascular endothelial cells 1).
In MICE, this cytotoxicity is used to selectively damage endothelial cells of corneal neovascularization. The hydrostatic pressure from MMC injection delivers MMC to both afferent and efferent vessels. Damage to vascular endothelial cells causes vascular occlusion, inducing regression of corneal neovascularization. By occluding the vessels that supply lipid deposits, improvement in lipid keratopathy is also expected.
Pathophysiological background of limitations of conventional treatment
Anti-VEGF therapy targets only VEGF-A, and the recruitment of pericytes around corneal neovascularization to form a barrier are factors that limit the efficacy of conventional treatment 1). Mature corneal neovessels are covered by pericytes, which attenuates the vascular regression effect of anti-VEGF drugs. MICE differs from conventional treatment in that it acts directly on endothelial cells from the vascular lumen without going through this barrier.
MICE is a new technique first reported by Dr. Ouano in 2022, and accumulation of clinical data has just begun.
Rangu et al. reported the world’s first case of MICE performed as a prophylactic treatment before penetrating keratoplasty (PKP) in a patient with corneal neovascularization due to herpes simplex virus-1 keratitis 1). After MICE, PKP was performed, and good visual acuity and non-recurrence of corneal neovascularization were confirmed for over one year 1). Since the rejection rate of corneal transplantation in eyes with corneal neovascularization is as high as 3–36% 1), prophylactic neovascular removal by MICE may contribute to improving transplant success rates.
Future challenges include the following:
Long-term safety evaluation: The effect of MMC on corneal endothelial cells is unknown, and serial evaluation by specular microscopy is recommended 1)
Optimization of indications: Establishment of appropriate candidate selection criteria is necessary
Large-scale clinical studies: Evaluation of long-term outcomes and adverse effect profiles is required
Combination with other treatments: Comparative studies with FND and anti-VEGF therapy, and investigation of combination therapy are expected
QWhat is the long-term safety of MICE?
A
MICE has only been reported recently, and long-term safety data are limited. In particular, the effect of MMC on corneal endothelial cells is unknown, and after MICE, serial evaluation of the corneal endothelium by specular microscopy or corneal confocal microscopy is recommended 1). No short-term adverse events have been reported at present, but future data accumulation is essential.
Rangu N, Riaz KM. Mitomycin intravascular chemoembolization (MICE) to treat corneal vascularization prior to penetrating keratoplasty. American journal of ophthalmology case reports. 2024;33:101993. doi:10.1016/j.ajoc.2024.101993. PMID:38298265; PMCID:PMC10828578.
Velazquez DC, Ortiz-Morales G, Vera-Duarte GR, Navas A, Ramirez-Miranda A, Graue-Hernandez EO. Mitomycin Intravascular Chemoembolization for Corneal Neovascularization. Cornea. 2024;44(8):965-969. PMID: 39177412.
Mimouni M, Ouano D. Initial outcomes of mitomycin intravascular chemoembolization (MICE) for corneal neovascularization. Int Ophthalmol. 2022;42(8):2407-2416. PMID: 35099664.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.