Ocular rosacea is the ocular type (subtype IV) of rosacea, a chronic inflammatory skin disease 1). It is characterized by telangiectasia, blepharitis, meibomian gland dysfunction (MGD), and keratitis, causing chronic inflammation of the ocular surface.
The global prevalence of rosacea is approximately 5.5%, and ocular symptoms are observed in 58–72% of patients 1). The typical age of onset is 25–55 years, and it is more commonly diagnosed in women. It is more frequent in Fitzpatrick skin types I–II (fair skin), but also occurs in individuals with darker skin 1).
Skin findings precede ocular symptoms in 53% of cases, simultaneous onset occurs in 27%, and ocular findings precede skin findings in 20% of cases 1). Therefore, it is important to recognize that ocular rosacea can develop even without skin symptoms. Pediatric cases (pediatric blepharokeratoconjunctivitis) have also been reported 1).
QCan ocular rosacea develop without skin rosacea?
A
Ocular findings precede skin findings in about 20% of all cases 1). Even without typical skin symptoms such as facial erythema or telangiectasia, it can present as chronic blepharitis or meibomian gland dysfunction. If ocular surface symptoms persist, the possibility of ocular rosacea should be considered.
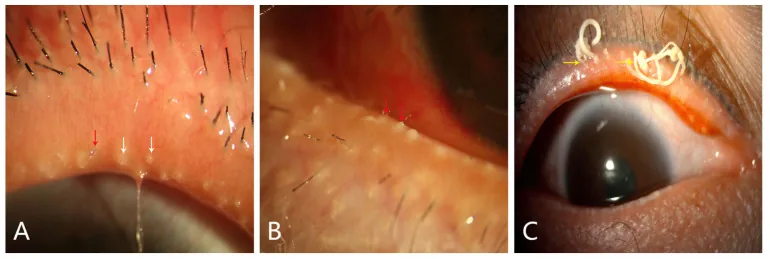
Ya-Li Du, Xi Peng, Yang Liu, Jia-Song Wang, et al. Ductal Hyperkeratinization and Acinar Renewal Abnormality: New Concepts on Pathogenesis of Meibomian Gland Dysfunction 2023 Feb 27 Curr Issues Mol Biol. 2023 Feb 27; 45(3):1889-1901 Figure 3. PMCID: PMC10047716. License: CC BY.
Images A and B show telangiectasia of the eyelid margin, crusting, and obstruction of meibomian gland openings. Image C shows cylindrical dandruff adhering to the eyelid margin, indicating posterior blepharitis and eyelid margin abnormalities associated with meibomian gland dysfunction.
Decreased vision: In cases of corneal infiltration or scarring
Symptoms tend to progress over time with repeated exacerbations and remissions 1). The severity of skin symptoms does not necessarily correlate with the severity of ocular symptoms.
Conjunctival injection: Redness of the bulbar conjunctiva. May be accompanied by follicular and papillary reactions 1).
Corneal lesions: Occur in 25–50% of cases. May progress from superficial punctate keratitis to marginal infiltration, neovascularization, ulceration, and perforation 1).
Corneal scarring: Persistent inflammation involving the visual axis can cause visual impairment.
Rare Findings
Morbihan syndrome: Indolent edema of the forehead, nose, glabella, cheeks, and periorbital area. Accompanied by lymphedema 5).
Rhinophyma: Late-stage skin finding. Thickening, nodularity, and fibrosis of the skin.
Non-invasive meibography is useful for morphological assessment of the meibomian glands. Meibography is the only method to observe meibomian gland structures in vivo using transillumination of the eyelids.
The exact cause of ocular rosacea is unknown, but it involves a combination of immune dysfunction, vascular dysregulation, microbial factors, and genetic predisposition 1).
Immune dysfunction: Overactivation of the innate immune system. Overexpression of TLR2 leads to increased KLK5, abnormal production of cathelicidin LL-37, elevated VEGF, and subsequent angiogenesis and inflammation 1)2).
Demodex mites: Present in high density in rosacea patients. The commensal bacterium Bacillus oleronius triggers an immune response, worsening ocular surface inflammation1)4)
Neurovascular dysregulation: Dysfunction of cutaneous nerves amplifies flushing and burning sensations1)
Genetic predisposition: HLA-related polymorphisms such as HLA-DRA and BTNLA2 have been reported1)
Environmental and lifestyle factors: Ultraviolet light, extreme temperatures and wind, alcohol, spicy foods, stress, and certain cosmetics or medications are exacerbating factors1)
Prolonged exposure to ultraviolet light, consumption of alcohol and caffeine, spicy foods and hot drinks, mental stress, intense exercise, and exposure to extreme temperatures and wind are typical exacerbating factors. These promote vasodilation and inflammation, triggering symptom recurrence. Since triggers vary by individual, keeping a daily log to identify personal triggers is recommended.
Ocular rosacea is a clinical diagnosis; there are no specific diagnostic tests1). The 2019 Global ROSacea COnsensus (ROSCO) panel recommends a comprehensive diagnostic approach1).
History taking: Nature and frequency of symptoms, exacerbating factors, presence of skin symptoms. Quantitative assessment using OSDI/SPEED questionnaires6)
Skin observation: Presence of erythema, telangiectasia, papules, and pustules on the central face (cheeks, nose, chin, forehead)
Slit-lamp examination: Vascular dilation, thickening, and irregularity of the eyelid margins; degree of meibomian gland dysfunction (quality and expressibility of meibum); conjunctival and corneal findings
Tear film tests: Tear break-up time (TBUT), fluorescein/lissamine green staining
Meibography: Morphological assessment of meibomian glands; quantification of dropout
Treatment of ocular rosacea is recommended with a stepwise approach based on severity 1). The ROSCO International Panel, the National Rosacea Society Expert Committee, and the Swiss treatment guidelines provide treatment recommendations.
Demodex removal with eyelid wipes containing terpinen-4-ol (T4O) is effective.
Yin et al. (2021) reported a case of a 72-year-old woman with refractory rosacea-related blepharitis over 5 years, treated with T4O wipes 4). Facial and eyelid erythema markedly improved within 1 month, and telangiectasia disappeared within 2 months. The OSDI score improved from 37 to 15, and complete Demodex eradication and symptom resolution were maintained over 8 months of follow-up.
In a systematic review by Shergill et al. (2024), IPL + MGX combination resulted in partial response in 91% (89/98) of cases 3). No complete remission was observed, but the frequency and severity of dry eye symptoms and eyelid margin redness were reduced. The Toyos protocol, consisting of 3–4 sessions at 4–6 week intervals, is commonly used.
Deep anterior lamellar keratoplasty (DALK) is recommended when corneal scarring involves the visual axis 1). Full-thickness corneal transplantation often has poor prognosis due to corneal neovascularization and chronic inflammation. Conjunctival flap, Tenon patch graft, and tissue adhesive are used for corneal perforation 1).
QWhat is IPL therapy?
A
IPL (Intense Pulsed Light) therapy is a treatment that uses pulsed light from a flash lamp applied to the face to improve meibomian gland secretion, reduce inflammation, and eliminate Demodex. It is performed with a protective shield placed over the eyelids, without direct irradiation of the eyelids. Typically, 3 to 4 sessions are conducted at intervals of 4 to 6 weeks. For details, refer to the IPL therapy section in Standard Treatments.
QCan ocular rosacea be cured?
A
Ocular rosacea is a chronic disease, and complete cure is difficult. The goal of treatment is to control symptoms and prevent complications. With continued eyelid hygiene and avoidance of exacerbating factors, a stable condition can often be maintained, but flare-ups of inflammation require appropriate medication.
The pathophysiology of ocular rosacea is a chronic inflammation involving complex interactions of excessive activation of the innate immune system, neurovascular dysregulation, and meibomian gland dysfunction1)2).
Overexpression of TLR2 in keratinocytes plays a central role1)2). TLR2 activates the NF-κB signaling pathway, inducing the production of inflammatory cytokines such as IL-1β, TNF-α, IL-6, and IL-8. At the same time, it promotes the production of cathelicidin LL-37 via the serine protease KLK52).
LL-37 maintains chronic inflammation through the following combined actions:
Promotion of leukocyte migration
Promotion of release of MMP-9, IL-6, and histamine from mast cells2)
Increased VEGF production in keratinocytes → angiogenesis and telangiectasia
In the tear fluid of patients with ocular rosacea, concentrations of IL-1α/β, MMP-8, and MMP-9 are elevated2). IL-1α promotes the production and activation of MMP-9, causing irritation symptoms of the eyelids and ocular surface, corneal epithelial defects, corneal ulcers, and corneal neovascularization2). The lower the tear clearance, the higher the concentration of these inflammatory factors.
MGD is defined as “a diffuse chronic abnormality of the meibomian glands, characterized by terminal duct obstruction and/or qualitative or quantitative changes in glandular secretion.” Obstruction occurs due to hyperkeratinization of the ductal epithelium and increased viscosity of meibum, leading to gland dropout, atrophy, and decreased secretion 2). Reduction of the lipid layer promotes tear evaporation, causing evaporative dry eye.
Meibomian gland dysfunction is broadly classified into hyposecretory and hypersecretory types, each with primary and secondary forms.
Demodex folliculorum and D. brevis parasitize sebaceous glands. In rosacea patients, they are present at higher densities than in normal skin, activating TLR2 and enhancing innate immune responses 4). Superantigens produced by the commensal bacterium Bacillus oleronius activate CD4+ T cells and macrophages via IL-8 and IL-12p70 production, promoting Langerhans cell infiltration 4). Demodex also increases the production of lipases and esterases, promoting lipid breakdown of meibum and worsening meibomian gland dysfunction.
7. Latest research and future perspectives (research-stage reports)
A review by Mohamed-Noriega et al. (2025) reports that with advances in understanding immune dysregulation and microbiome changes, exploration of targeted therapies including biologics and small molecule inhibitors is progressing 1). Specific drug names and clinical trial results have not yet been sufficiently accumulated.
It has been suggested that gut dysbiosis may be involved in the exacerbation and recurrence of rosacea 1). Elucidation of inflammatory pathways via the gut-eye axis may lead to the discovery of new therapeutic targets.
Genome-wide association studies (GWAS) have reported that single nucleotide polymorphisms in HLA-DRA, BTNLA2, HLA-DRB1*03:01, etc., are associated with rosacea 1). Elucidation of genetic predisposition may form the basis for personalized treatment.
Anti-VEGF eye drops or subconjunctival injections are being considered for the management of corneal neovascularization1). Fine-needle diathermy for existing telangiectasias has also been reported as an option.
Mohamed-Noriega K, Loya-Garcia D, Vera-Duarte GR, Morales-Wong F, Ortiz-Morales G, Navas A, et al. Ocular Rosacea: An Updated Review. Cornea. 2025;44(4):525-537. doi:10.1097/ICO.0000000000003785. PMID:39808113; PMCID:PMC11872267.
Rodrigues-Braz D, Zhao M, Yesilirmak N, Aractingi S, Behar-Cohen F, Bourges JL. Cutaneous and ocular rosacea: Common and specific physiopathogenic mechanisms and study models. Molecular vision. 2021;27:323-353. PMID:34035646; PMCID:PMC8131178.
Shergill M, Khaslavsky S, Avraham S, Kashetsky N, Zaslavsky K, Mukovozov I. A Review of Intense Pulsed Light in the Treatment of Ocular Rosacea. Journal of cutaneous medicine and surgery. 2024;28(4):370-374. doi:10.1177/12034754241254051. PMID:38804504; PMCID:PMC11403922.
Yin HY, Tighe S, Tseng SC, Cheng AM. Successful management of chronic Blepharo-rosacea associated demodex by lid scrub with terpinen-4-ol. American journal of ophthalmology case reports. 2021;23:101171. doi:10.1016/j.ajoc.2021.101171. PMID:34368495; PMCID:PMC8326346.
Li SWR, Clancy N, Intzedy L, Stone N, Obi E. Unilateral Peri-Orbital Oedema and Mechanical Ptosis: An Unusual Case Presentation of Rosacea. Case reports in ophthalmology. 2025;16(1):677-685. doi:10.1159/000548178. PMID:41058755; PMCID:PMC12500299.
Khadamy J. Ocular Rosacea: Don’t Forget Eyelids and Skin in the Assessment of This Stubborn Ocular Surface Disease. Cureus. 2024;16(1):e51439. doi:10.7759/cureus.51439. PMID:38298298; PMCID:PMC10828744.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.