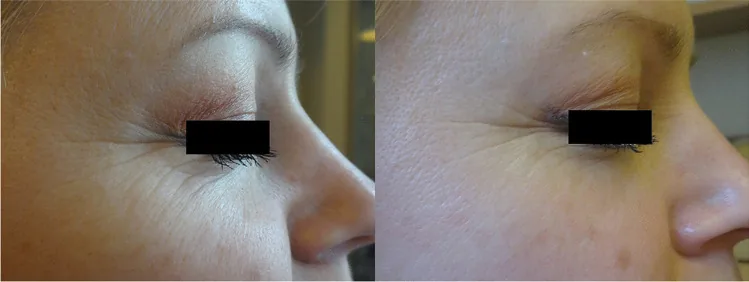
Anna Kołodziejczak, Helena Rotsztejn Efficacy of fractional laser, radiofrequency and IPL rejuvenation of periorbital region 2021 May 14 Lasers Med Sci. 2022 May 14; 37(2):895-903 Figure 4. PMCID: PMC8918123. License: CC BY.
Left: before IPL; right: after treatment, showing reduction of fine wrinkles on the skin from the lower eyelid to the outer canthus. This is a before-and-after comparison photograph of the periorbital skin appearance.
Intense pulsed light (IPL) therapy is a treatment that delivers non-coherent, non-collimated, high-energy polychromatic light in the wavelength range of 500–1200 nm. In dermatology, it has been used for many years to treat telangiectasia in rosacea and pigmented lesions3).
IPL light can selectively target specific tissues or chromophores by using appropriate filters to exclude unwanted wavelengths. Fluence is adjusted in the range of 3–40 J/cm², and pulse duration in the range of 10–340 ms. Pulses are delivered as single, double, or triple pulses.
In IPL treatment, the eyes are protected with opaque goggles, and ultrasound gel is applied to the periorbital skin. The standard irradiation areas are the skin below the lower eyelids and both cheeks 2).
Parameter
Adjustment Criteria
Wavelength filter
Selected according to skin type
Fluence
12–19 J/cm²
Number of pulses
Adjusted based on degree of pigmentation
Irradiation parameters are adjusted based on the Fitzpatrick classification. Skin types I–IV are suitable 1). Types V–VI are contraindicated due to the risk of excessive reaction to skin pigment 1).
A standard protocol consists of 4 treatments at 2–4 week intervals 1). Mechanical expression of meibomian glands (MGX) is often performed after each session 1).
There are reports that additional irradiation to the upper eyelids results in greater improvement of dry eye symptoms compared to irradiation of the lower eyelids alone 2).
QIs IPL treatment painful?
A
IPL treatment may be accompanied by a mild sensation of warmth or a snapping rubber band feeling, but severe pain usually does not occur. Irradiation is performed while cooling the skin with a sapphire contact surface. Mild redness or swelling may occur after treatment, but the frequency is about 13%, and no serious side effects have been reported.
Low-level light therapy (LLLT) combined with other treatments shows synergistic effects in meibomian gland dysfunction treatment 2). In a combination treatment using the Eye-light® device, 70% of 460 eyes showed improvement of at least one grade in meibomian gland dysfunction severity 2). The proportion of eyes with TBUT ≤6 seconds before treatment was 86.7%, which decreased to 33.9% after treatment 2).
Radiofrequency (RF) + IPL + MGX triple combination therapy has also been reported 1). In a prospective study of 31 patients, modified MGS decreased by 69.3% (p<0.0001) and OSDI decreased by 60.7% (p<0.0001) 1). The addition of RF resulted in significantly greater improvement in mMGS compared to IPL+MGX alone 1). Additionally, the mucosal pemphigoid-9 positivity rate decreased from 66.1% at baseline to 32.3% after treatment 1).
In the IPL+MGX combination group, significant decreases in IL-6, IL-6R, IL-1β, IL-13, and CCL11/Eotaxin were observed compared to the warm compress+MGX group 2). Tear levels of IL-17α and IL-6 also significantly decreased after IPL treatment 3).
QHow many IPL treatments are needed?
A
The standard protocol consists of 4 treatment sessions at 2–4 week intervals. Many clinical studies report significant improvement after 4 sessions. However, the effect is not permanent; some reports indicate that the effect diminishes after 9 months, so regular maintenance sessions may be necessary.
The exact mechanism by which IPL improves meibomian gland dysfunction and dry eye is not fully understood, but several mechanisms have been proposed 2)3).
Selective photothermolysis is considered the primary mechanism of action of IPL 2). The light is absorbed by oxyhemoglobin in blood vessels and converted to heat 3). This causes thrombosis and occlusion of abnormal telangiectasias around the eyelids, removing the source of inflammatory mediators 3).
Warming and liquefaction of meibum is also an important effect of IPL 3). In meibomian gland dysfunction, the ducts are obstructed by keratinized cellular components and viscous meibum. The thermal effect of IPL liquefies the meibum, facilitating its expression and drainage 3).
Proposed mechanisms of IPL action include thrombus formation in abnormal vessels, warming of meibomian glands, activation of fibroblasts, reduction of bacterial load, modulation of anti-inflammatory agents, and changes in reactive oxygen species levels. 2)
Other suggested mechanisms include: suppression of secondary inflammation by killing Demodex mites3). Improvement of dermal connective tissue through activation of fibroblasts and promotion of collagen synthesis has also been reported. Indirect suppression of inflammatory cytokines and mucous membrane pemphigoid production via downregulation of TNF-α has been suggested. Neurotrophic effects on the cornea and ocular surface have also been reported, and the improvement of symptoms as early as 2 hours after IPL suggests this neurological effect.
QHow does IPL improve dry eye?
A
IPL improves dry eye through multiple mechanisms. The primary action is the destruction of abnormal telangiectasia around the eyelids by photothermolysis, blocking the supply of inflammatory mediators to the meibomian glands. Additionally, warming and liquefaction of meibum, killing of Demodex, reduction of inflammatory cytokines (e.g., IL-6, IL-17α), and promotion of collagen synthesis via fibroblast activation are involved. These combined effects improve meibomian gland dysfunction and stabilize the lipid layer of the tear film.
The application range of IPL treatment is expanding. In a clinical trial of prophylactic IPL during the perioperative period of refractive surgery, the IPL group showed significantly better results in OSDI, NIBUT, TMH, and meibography compared to the sham group 2). However, the difference in OSDI diminished after 6 months 2).
The efficacy of IPL combined with LLLT for dry eye in Sjögren’s syndrome has also been reported 2). There are also studies showing the usefulness of IPL treatment for meibomian gland dysfunction in patients using glaucoma eye drops2).
The triple combination of RF + IPL + MGX is expected as a new treatment strategy 1). The addition of RF increased improvement in meibum quality and also showed a decrease in the MMP-9 positivity rate 1). However, randomized controlled trials are needed in the future to clarify the independent contribution of RF 1).
Most studies show that IPL improves symptoms and signs of dry eye associated with meibomian gland dysfunction, but the degree and duration of efficacy vary greatly depending on combination therapy and number of treatments. Independent large-scale randomized controlled trials are still needed. 2)
Establishing the optimal treatment regimen, determining the duration of effect, and identifying the patient groups that benefit most are future challenges 2). Further investigation is also required on the impact of differences in algorithms and light characteristics among different IPL devices on treatment outcomes 2).
Chelnis J, Garcia CN, Hamza H. Multi-Frequency RF Combined with Intense Pulsed Light Improves Signs and Symptoms of Dry Eye Disease Due to Meibomian Gland Dysfunction. Clinical ophthalmology (Auckland, N.Z.). 2023;17:3089-3102. doi:10.2147/OPTH.S426564. PMID:37881780; PMCID:PMC10595163.
TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;279:295-380.
Sabeti S, Kheirkhah A, Yin J, Dana R. Management of Meibomian Gland Dysfunction: a review. Surv Ophthalmol. 2020;65(2):205-217.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.