Perfluorohexyloctane (PFHO) ophthalmic solution (brand name: Miebo®, Bausch+Lomb) was approved by the FDA in May 2023 for the treatment of signs and symptoms of dry eye disease (DED). It is the first FDA-approved prescription eye drop targeting tear evaporation 2).
PFHO is an amphiphilic semifluorinated alkane (chemical formula C₁₄H₁₇F₁₃, F6H8) with a lipophilic hydrocarbon segment and a lipophobic fluorocarbon segment 3). This formulation is a single-component, water-free, preservative-free preparation consisting of 100% active ingredient 4). In the US, it is sold as a prescription drug, but in Europe, Australia, and New Zealand, it has been used for several years under the names EvoTears®/NovaTears® 4).
Dry eye is a multifactorial disease affecting over 16 million people in the US, with increased tear evaporation contributing to up to 90% of cases 3). Meibomian gland dysfunction (MGD) is the leading cause of evaporative dry eye1).
QHow is PFHO different from other dry eye treatments?
A
Existing FDA-approved DED prescription drugs such as cyclosporine (Restasis®, Cequa®) and lifitegrast (Xiidra®) improve tear production through anti-inflammatory effects. Varenicline (Tyrvaya®) stimulates tear secretion by targeting the parasympathetic pathway. In contrast, PFHO has a completely different mechanism of action, forming an anti-evaporation layer on the tear film surface, and is the first prescription eye drop specifically for evaporative dry eye.
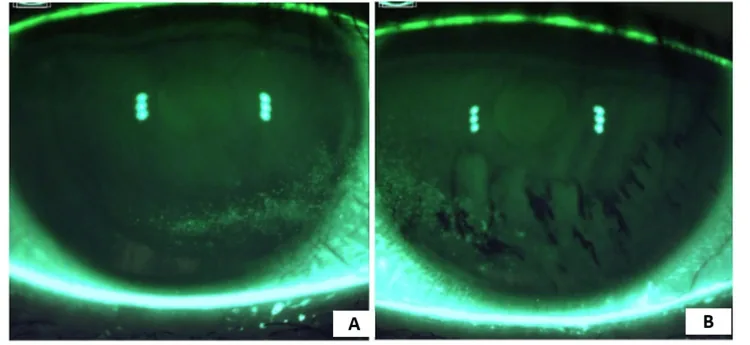
Cureus. 2025; 17(2):e78554. Figure 2. PMCID: PMC11887804. License: CC BY.
Slit-lamp photograph under fluorescein staining, showing corneal surface staining and tear film changes that can be compared between the right and left eyes. Corneal epithelial damage and changes before and after treatment are depicted.
Shortened tear film break-up time (BUT): In Japanese diagnostic criteria, BUT ≤5 seconds is a requirement for definitive diagnosis
Positive corneal fluorescein staining: reflects the degree of corneal epithelial damage. Total corneal fluorescein staining score (tCFS) is used as a primary endpoint in clinical trials
Meibomian gland dysfunction (MGD): the leading cause of evaporative dry eye. Obstruction of the terminal ducts of the meibomian glands or qualitative changes in gland secretion lead to dysfunction of the tear lipid layer1)
According to the diagnostic criteria of the Japanese Dry Eye Society, a definitive diagnosis is made when both subjective symptoms and a tear break-up time (BUT) of 5 seconds or less are present. According to the TFOS DEWS II definition, loss of tear film homeostasis, increased tear osmolarity, ocular surface inflammation, and neurosensory abnormalities also play etiological roles.
Tear film breakup time (BUT): Measures the time until the tear film first breaks after fluorescein staining.
Schirmer test: Quantitatively evaluates tear secretion. A value of 5 mm or less without anesthesia suggests aqueous tear deficiency.
Meibomian gland evaluation: Assesses gland morphology, expressibility of secretions, and meibum quality.
Tear film oriented diagnosis (TFOD): Identifies the causative layer by the tear film breakup pattern immediately after eye opening.
QWhich patients are suitable for PFHO?
A
PFHO is particularly suitable for patients with evaporative dry eye associated with MGD. In clinical trials, patients with BUT ≤5 seconds, Schirmer test ≥5 mm, MGD score ≥3, and tCFS 4–11 were included. For aqueous tear-deficient dry eye with markedly reduced tear secretion, cyclosporine ophthalmic solution, an immunomodulator, may be appropriate.
PFHO is a preservative- and additive-free ophthalmic solution consisting of 100% perfluorohexyloctane. The recommended dose is one drop in each affected eye four times daily.
In two Phase 3 randomized double-blind trials (GOBI and MOJAVE), PFHO administered four times daily significantly improved both primary endpoints, tCFS and VAS dryness score, compared to saline control at week 8 4).
A meta-analysis of 4 RCTs (1,814 patients) reported the following results 1):
The PFHO group significantly improved tCFS compared to the control group (MD -1.09; 95% CI -1.37 to -0.82; P < 0.001; I² = 0%). Eye distress VAS (MD -9.69; P < 0.01), OSDI (MD -5.79; P < 0.01), and burning/stinging score (MD -7.16; P < 0.01) were also significantly improved, with no heterogeneity observed 1).
In the KALAHARI trial (208 patients, 52 weeks), an extension of the GOBI trial, the mean change from baseline in tCFS was -2.1 and the mean change in VAS dryness score was -33.7, confirming sustained efficacy over 60 weeks 4).
Trial
Subjects
tCFS Improvement (LSMD)
VAS Improvement (LSMD)
GOBI
597 patients
-0.97 (P < 0.001)
-7.6 (P < 0.001)
MOJAVE
620 patients
-1.2 (P < 0.001)
-10.2 (P < 0.001)
Significant improvements in tCFS and VAS dryness score were already observed at week 2 (day 15), and symptom improvement was also observed at 5 minutes after a single instillation 4).
Most common adverse event: blurred vision (1.3–3.0%). Mild and transient 4)
Incidence of ocular adverse events: No significant difference between PFHO and control groups (RR 1.00; 95% CI 0.77–1.29; P = 0.999) 1)
Serious ocular adverse events: None reported across the GOBI, MOJAVE, and KALAHARI trials 3)
Discontinuation rate: Low 3)
Nonclinical studies have confirmed non-toxicity and non-bioaccumulation 4)
PFHO currently has no absolute contraindications, but its safety and efficacy in pregnant women, nursing mothers, and individuals under 18 years of age have not been established.
In Japan, treatment is performed based on the concept of “Tear Film Oriented Therapy (TFOT)” advocated by the Dry Eye Society, targeting the causative layer. For the lipid layer, warm compresses and eyelid hygiene are used; for the aqueous layer, sodium hyaluronate and punctal plugs; for secretory mucin, diquafosol sodium; and for the epithelium, rebamipide. PFHO may serve as a new option that directly suppresses tear evaporation by complementing lipid layer function.
QAre there side effects?
A
The most commonly reported side effect in clinical trials was blurred vision (1.3–3.0%), which was mild and transient. Other reported side effects include blepharitis, conjunctival hyperemia, conjunctival papillae, and instillation site pain, all of which are infrequent. Meta-analysis has shown that the incidence of ocular adverse events is comparable between the PFHO and control groups.
QHow quickly does the effect appear?
A
In clinical trials, symptom improvement was observed as early as 5 minutes after a single instillation. By week 2 (day 15), significant improvements were confirmed in both corneal fluorescein staining scores and dryness scores. In the KALAHARI extension study, the effect was sustained for up to 52 weeks.
The core of dry eye pathophysiology is tear hyperosmolarity 2). When tear osmolarity increases due to reduced tear secretion or increased evaporation, it triggers MAP kinase activation and secretion of inflammatory cytokines, chemokines, and matrix metalloproteinases 2). These inflammatory mediators induce apoptosis of corneal epithelial cells, conjunctival cells, and goblet cells, leading to glycocalyx damage, reduced ocular surface lubrication, and tear film instability. This results in further hyperosmolarity, forming a “vicious circle” 2).
Several mechanisms have been proposed for the action of PFHO 4).
Inhibition of tear evaporation is the primary mechanism. PFHO is an amphiphilic molecule that self-assembles at the tear-air interface, forming an ordered monolayer due to its fluorocarbon segment (oleophobic, air-loving) and hydrocarbon segment (lipophilic) 3). This monolayer physically suppresses evaporation of the aqueous tear layer. In vitro, applying PFHO to saline reduces evaporation by approximately 80% 2).
In an in vitro gravimetric analysis comparing evaporation rates of PFHO and PFBP (perfluorobutylpentane), PFHO evaporated less than 1.5% after 1 hour, whereas PFBP evaporated 93%. In an ex vivo model, corneal retention of PFHO after 1 hour was 54.5%, about three times that of PFBP (18.6%) 3).
Reduction of corneal surface temperature and TRPM8 activation is the second mechanism 4). Topical application of PFHO lowers corneal surface temperature and increases the activity of corneal TRPM8 cold receptors. This response is thought to promote reflex tearing and blinking, and reduce discomfort and pain.
Improvement of the tear lipid layer has also been reported. Preclinical data show that after 7 days of PFHO administration, lipid layer grade improved as early as 5 minutes after a single instillation, and the improvement was maintained for 5–7 days with repeated dosing 4). Clinical trials have also observed improvements in lipid layer thickness and tear film thickness at 4 weeks 4).
In the TFOS DEWS III Management and Therapy Report published in 2025, PFHO is positioned as an evidence-based treatment option for evaporative dry eye disease (DED) 4). A systematic review (6 RCTs) reported that the PFHO group showed greater improvement than the control group in most variables including OSDI, lipid layer thickness, corneal staining, and adverse events 4).
Comparison of PFHO and Water-Free Cyclosporine 0.1%
Both PFHO and water-free CsA 0.1% (Vevye®) are SFA-containing, water-free, preservative-free formulations. However, PFHO targets evaporation suppression, while CsA 0.1% targets increased tear production through immunomodulation 3). In clinical trials, PFHO was studied in evaporative DED (with MGD), whereas CsA 0.1% trials excluded MGD and included severe cases of aqueous-deficient DED4).
The follow-up period in clinical trials was mainly 8 weeks, and long-term (over 1 year) efficacy and side effect evaluation is needed 1). Evaluation in patient groups excluded from trials, such as those with severe DED (tCFS > 11) or contact lens wearers, is also a future challenge 1). Approval in Japan is also anticipated.
Guedes J, Hespanhol LC, Freitas MAA, Balieiro CCA, Souza MEC, Faneli AC, et al. Efficacy and Safety of Perfluorohexyloctane in Evaporative Dry Eye Disease Associated With Meibomian Gland Dysfunction: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cureus. 2024;16(8):e67920. doi:10.7759/cureus.67920. PMID:39206330; PMCID:PMC11357713.
Azhar A, Taimuri MA, Oduoye MO, Sumbal A, Sheikh A, Iqbal A, et al. MEIBO (perfluorohexyloctane): a novel approach to treating dry eye disease. Annals of medicine and surgery (2012). 2024;86(9):5292-5298. doi:10.1097/MS9.0000000000002322. PMID:39239035; PMCID:PMC11374244.
Periman LM, White DE, Katsev D. Differentiating Between Perfluorohexyloctane Ophthalmic Solution and Water-Free Cyclosporine Ophthalmic Solution 0.1% for Dry Eye Disease: A Review of Preclinical and Clinical Characteristics. Ophthalmol Ther. 2025;14(2):283-293.
TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;279:289-386.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.