Drug-induced corneal complications are a general term for corneal disorders caused by topically administered (eye drops) or systemically administered drugs. Damage can occur in any layer of the cornea: the epithelium, stroma, or endothelium1).
The pathophysiology is broadly divided into the following three categories.
Drug Deposition
Epithelial deposition: Highly lipophilic drugs accumulate within the epithelium, forming vortex-shaped or linear opacities.
Stromal deposits: Components leaking from the limbal vascular network deposit in the stroma.
Endothelial deposits: Drugs accumulated in the aqueous humor adhere to the endothelial surface.
Cytotoxicity
Active ingredients of eye drops: Direct toxicity of antibiotics, antifungals, NSAIDs, beta-blockers, topical anesthetics, etc.
Preservatives: Benzalkonium chloride (BAK) is used in about 70% of ophthalmic preparations and causes cytotoxicity (cell death, tight junction disruption, apoptosis, immune-inflammatory response) in conjunctival and corneal epithelial cells2).
Systemic medications: Anticancer drugs transfer into the tear fluid and damage the corneal epithelium.
Allergy
Immediate type: Conjunctival hyperemia and edema appear within hours after instillation and resolve spontaneously in 2–3 days.
Delayed type: Progresses chronically as contact dermatitis or drug-induced pseudopemphigoid.
Topical medications act directly on the cornea. Systemic medications reach the cornea via the tear film, aqueous humor, and angle vasculature. Corneal drug deposits may be a precursor to retinal disease, making systemic evaluation important.
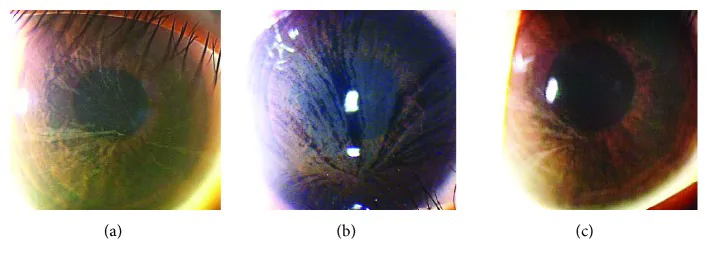
Yasuhito Ikegawa, Atsushi Shiraishi, Yasuhito Hayashi, Akiyoshi Ogimoto, et al. In Vivo Confocal Microscopic Observations of Vortex Keratopathy in Patients with Amiodarone-Induced Keratopathy and Fabry Disease 2018 Mar 21 J Ophthalmol. 2018 Mar 21; 2018:5315137 Figure 4. PMCID: PMC5884153. License: CC BY.
Three images showing ocular findings in patients with Fabry disease: (a) 32-year-old mother, (b) 8-year-old daughter, (c) 4-year-old daughter.
Corneal epithelial damage due to drug toxicity progresses in stages depending on severity.
Mild to Moderate
Superficial punctate keratitis (SPK): Initially appears in the central to inferior cornea, along the palpebral fissure. Diffuse SPK across the entire cornea suggests highly toxic drugs such as aminoglycosides.
Vortex keratopathy (cornea verticillata): Cationic amphiphilic drugs (e.g., amiodarone, hydroxychloroquine, tamoxifen, chlorpromazine) accumulate in the lysosomes of the corneal epithelial basal layer, forming vortex-shaped deposits along the centrifugal migration pattern of epithelial cells from the limbus to the central cornea1). It occurs in 98% of patients on amiodarone (200–300 mg/day) and in 100% of patients on hydroxychloroquine (800 mg/day) by 48 months 1).
Severe
Epithelial crack line: Crack-like opacities resulting from breakdown of compensatory changes. This is the stage immediately preceding epithelial defect.
Persistent epithelial defect: The proliferative capacity of basal cells and limbal stem cells has reached its limit.
Limbal stem cell deficiency: Long-term cytotoxicity damages the entire limbal stem cell population, leading to conjunctivalization of the cornea, the most severe form.
In drug-induced toxic keratopathy, corneal epithelial damage is more prominent than conjunctival epithelial damage. In contrast, dry eye disease typically presents with conjunctival epithelial damage first, which is a key differentiating point. Fluorescein staining shows characteristic late staining (baseline corneal staining) due to impaired epithelial barrier function.
QIf vortex keratopathy is found, what should be checked first?
A
First, taking a medication history is most important. Check for systemic drugs such as amiodarone, hydroxychloroquine, and indomethacin, as well as the use of multiple eye drops. Since Fabry disease also presents similar corneal findings, evaluate family history and skin/kidney symptoms for differential diagnosis.
Lipophilic drugs deposit within the epithelium, forming whorl-like opacities (cornea verticillata). Since these findings resemble those of Fabry disease, obtaining a medication history is essential for diagnosis.
Drug Class
Representative Drugs
Notes
Antiarrhythmics
Amiodarone
Nearly 100% at high doses
Antimalarials
HCQ, Chloroquine
Also watch for retinopathy
NSAIDs
Indomethacin
Whorl-like to linear
Other drugs such as tamoxifen, naproxen, atovaquone, suramin, clofazimine, and gold compounds can also cause vortex keratopathy.
Toxicity from eye drops: Preservatives (BAC) are the most common cause. The active ingredients of beta-blockers, prostaglandin analogs, NSAID eye drops, and aminoglycoside antibiotics also have epithelial toxicity. The more frequent the instillation and the more types used, and the longer the use, the more likely damage occurs.
Toxicity from anticancer drugs: Anticancer drugs that transfer into tears damage the corneal epithelium. Because EGFR and HER2 are expressed on the corneal epithelium, drugs targeting these have a high risk of epithelial damage.
TS-1 (tegafur, gimeracil, oteracil potassium): Damage tends to occur from the superior limbus, often accompanied by limbal stem cell damage. Lacrimal duct obstruction may also occur.
Rifabutin: Accumulates in the aqueous humor due to high lipophilicity, forming stellate refractive endothelial deposits
Amantadine: Causes corneal epithelial edema and a decrease in corneal endothelial cells
Phenothiazines: Cause endothelial damage via phototoxicity of the drug in the anterior chamber or cAMP-mediated mechanisms. If irreversible endothelial dysfunction occurs, it may progress to bullous keratopathy
QDoes corneal deposition due to amiodarone affect vision?
A
Amiodarone keratopathy usually does not affect vision. Brown, vortex-shaped deposits are seen in the deep corneal epithelium, but most cases are asymptomatic. Rarely, patients may complain of photophobia or halos. The cornea clears 3 to 20 months after discontinuation of the drug. However, because amiodarone has also been reported to cause ischemic optic neuropathy, if there is vision loss, optic nerve evaluation should also be performed.
The most important diagnostic step is taking a detailed medication history. Check both eye drops (type, frequency, duration of use, presence of preservatives) and systemic medications.
Evaluate the location and characteristics of drug deposits. Differentiate whether they are intraepithelial, subepithelial, or at what depth in the stroma.
Drug-induced whorl keratopathy must be differentiated from Fabry disease. Fabry disease is accompanied by systemic symptoms such as family history, angiokeratoma, renal impairment, and limb pain.
The principle of treatment is discontinuation or dose reduction of the suspected causative drug. However, if discontinuation is difficult due to treatment of the underlying disease (e.g., anticancer drugs or glaucoma medications), collaboration with the primary physician is necessary.
Preservative-free artificial tears: Dilute drug concentration on the corneal surface and maintain lubrication. Used to wash out drug in tears for epithelial damage caused by anticancer drugs.
If inflammation with hyperemia and follicular conjunctivitis is prominent due to toxicity, consider steroid eye drops. However, be aware of the effects of preservatives and delayed wound healing caused by steroids.
Topical administration: Eye drops come into direct contact with the corneal epithelium via the tear film. In addition to the cytotoxicity of the active ingredient, preservatives (e.g., BAC) damage the epithelial cell membrane.
Systemic administration: Drugs reach the cornea via three routes.
Via the tear film: Secreted from the blood into the tear fluid via the lacrimal gland. Anticancer drugs (e.g., TS-1) cause epithelial damage through this route
Via the aqueous humor: Drugs that cross the blood-aqueous barrier penetrate the cornea from the endothelial side. Rifabutin endothelial deposits occur via this mechanism
Via the angle vasculature: Components leaking from the limbal vascular network deposit in the stroma
Lipophilic drugs (e.g., amiodarone, chloroquine, indomethacin) tend to accumulate in the corneal epithelium. They form whorl-like deposits in the deep epithelial layer, clinically resembling cornea verticillata in Fabry disease. Amiodarone keratopathy is classified into grades I–IV by Orlando and correlates with dose and duration of therapy.
EGFR and HER2 are expressed in the corneal epithelium. Anticancer drugs targeting these receptors (e.g., cetuximab, erlotinib, trastuzumab) directly inhibit corneal epithelial proliferation and differentiation, leading to a high risk of epithelial damage.
QWill changing to preservative-free eye drops improve corneal damage?
A
If preservatives are the main cause, improvement can be expected2). Several strategies exist, including alternative preservatives (SofZia, Polyquad, Purite), preservative-free formulations, and sustained-release formulations2). However, if the toxicity is due to the active ingredient itself, switching to preservative-free formulations may not provide sufficient improvement. Improvement often takes weeks to months, and it is important not to rush into adding or changing treatments.