Associated Systemic Diseases
Turner syndrome: accompanied by lymphedema
Klippel-Trénaunay-Weber syndrome: vascular malformation
Nonne-Milroy-Meige disease: hereditary lymphedema
Lymphedema with distichiasis: conjunctival and peripheral lymphedema

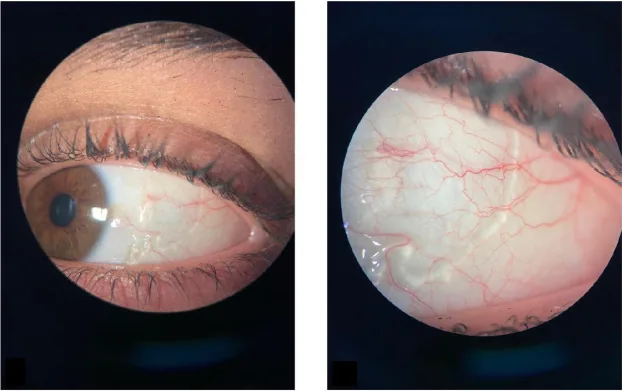
Conjunctival lymphangiectasia (CL) is a disease in which the lymphatic vessels of the conjunctiva become focally and abnormally dilated, presenting as localized edematous elevations on the conjunctiva. The conjunctival lymphatics are responsible for draining excess fluid and waste from the ocular surface, and their dilation can cause hyperemia, swelling, irritation, and epiphora.
| Type | Features |
|---|---|
| Diffuse type | Widespread conjunctival edema |
| Localized type | String of pearls appearance |
| Hemorrhagic | Blood filling within lymphatic vessels |
In the localized type, small translucent bumps arranged in a beaded pattern are characteristic, described as a “string of pearls.” Hemorrhagic conjunctival lymphangiectasia is a condition in which communications form between dilated lymphatic vessels and blood vessels, leading to intermittent blood filling within the lymphatic vessels.
The prevalence in the general population is approximately 1%. It is significantly higher in patients with hereditary transthyretin amyloidosis, and it has been suggested that it may serve as a biomarker for severe systemic disease.
Conjunctival lymphangiectasia is a localized dilation of lymphatic vessels, while lymphangiocyst is a cystic form of dilated lymphatic vessels. Pathologically, they lie on the same spectrum, and it may be difficult to distinguish between them. If there is a beaded appearance or repeated episodes of bleeding and resolution, lymphangiectasia is more likely.
Often asymptomatic. When symptoms are present, patients complain of foreign body sensation, hyperemia, and tearing. In the hemorrhagic type, bloody discharge may be observed. Some patients visit due to cosmetic concerns.
Slit-lamp examination reveals translucent to yellowish edematous elevations on the bulbar conjunctiva. In the localized type, small beaded elevations (string of pearls appearance) are characteristic. The diffuse type presents with extensive conjunctival edema (chemosis).
In the hemorrhagic type, blood fills the dilated lymphatic vessels, and a pseudohypopyon-like horizontal level may form within the cyst. Communication with veins becomes apparent after trauma or inflammation.
Chronic inflammation, scarring after eye surgery or trauma, and impaired lymphatic circulation are suspected causes. It may also occur idiopathically, and the mechanism of onset is not fully understood.
Lymphangiectasia in infancy results from underdevelopment of the lymphatic system and is often associated with the following systemic diseases.
Associated Systemic Diseases
Turner syndrome: accompanied by lymphedema
Klippel-Trénaunay-Weber syndrome: vascular malformation
Nonne-Milroy-Meige disease: hereditary lymphedema
Lymphedema with distichiasis: conjunctival and peripheral lymphedema
Associated Metabolic Diseases
Fabry disease: In classic Fabry disease, the prevalence of CL is high (approximately 80–85%) even under enzyme replacement therapy, and it has been reported that it may serve as a biomarker for undiagnosed cases 1)
Hereditary transthyretin amyloidosis: prevalence is significantly higher than in the general population 1)
If conjunctival lymphangiectasia is found in an infant, a thorough systemic examination is necessary to rule out systemic disease.
Evaluate the morphology, distribution, and color of edematous elevations on the conjunctiva. Findings such as bead-like chains or repeated resolution and recurrence of hemorrhage suggest this disease.
Low-reflectance cystic lesions of various sizes are observed. It can noninvasively assess the extent and degree of lymphatic dilation and is useful for confirming the diagnosis as “fluid-filled dilated lymphatic vessels” without the need for biopsy 2).
Definitive diagnosis is based on pathological findings. Dilated lymphatic vessels are lined by a single layer of endothelial cells, with lymph fluid accumulation in the lumen.
| Differential Disease | Key Differentiating Points |
|---|---|
| Conjunctival Inclusion Cyst | Solitary, spherical, mobile |
| Lymphangioma | Multilocular, deep infiltration |
| Allergic conjunctivitis | Redness, itching, papillae |
Differential diagnoses include conjunctivochalasis, pinguecula, conjunctival intraepithelial neoplasia, and conjunctival nevus cyst. A bead-like appearance with recurrent bleeding and resolution is highly suggestive of this condition.
Blister-like swelling of the conjunctiva can be caused by various conditions including conjunctival lymphangiectasia, conjunctival inclusion cyst, chemosis, and allergic conjunctivitis. It may resolve spontaneously, but if it persists or is accompanied by bleeding, an ophthalmologic examination is recommended.
Many cases of conjunctival lymphangiectasia resolve spontaneously without intervention. If asymptomatic, observation is sufficient.
If the patient complains of a foreign body sensation or experiences recurrent bleeding, eye drops are used. A combination of artificial tears (e.g., Soft Santear 6 times daily) and low-potency steroid eye drops (e.g., Flumetholon 0.1% twice daily, tapered as improvement occurs) is a typical prescription. Antihistamine eye drops may also be used.
Surgery is indicated when eye drops are insufficient or for cosmetic concerns.
Surgical Excision
Procedure: Lesion excision followed by conjunctival autograft or amniotic membrane transplantation
Features: Lowest recurrence rate
Indications: Cases resistant to drug therapy
Cryotherapy
Method: Freezing with liquid nitrogen
Features: Effective as an alternative to surgical excision
Note: Multiple sessions may be required for optimal results
A single subconjunctival injection of anti-VEGF agent (bevacizumab) targets VEGF involved in lymphangiogenesis, and its efficacy has been reported3). In a case report by Tan et al. (2016), conjunctival edema improved 5 days after injection, and symptoms completely resolved at 1 month3). High-frequency electrocautery preserves more conjunctival tissue than surgical excision and is gaining attention as a first-line treatment option4).
Many cases of conjunctival lymphangiectasia resolve spontaneously. If asymptomatic, observation alone is sufficient. However, if symptoms persist or bleeding recurs, eye drops or surgery may be necessary. Recurrence is usually not seen after complete excision.
The conjunctival lymphatic vessels are more developed than in other ocular tissues, and the lamina propria of the bulbar conjunctiva consists of loose connective tissue, making it highly mobile. In lymphangiectasia, the wall structure of the lymphatic vessels becomes fragile due to some cause, and the lumen dilates due to increased internal pressure or impaired drainage of lymph fluid.
When a communication forms between dilated lymphatic vessels and veins at the site of vascular malformation, blood flows into the lymphatic vessels. Trauma or inflammation often triggers the manifestation of this communication. The blood accumulated in the lymphatic vessels settles due to gravity, forming a horizontal level resembling pseudohypopyon.
Congenital conjunctival lymphangiectasia results from lymphatic system hypoplasia. In Turner syndrome and Klippel-Trenaunay-Weber syndrome, conjunctival lesions appear as part of systemic lymphatic malformations.