Surgery-related
Strabismus surgery: incidence 0.25–2.3%4)9)
Glaucoma surgery: can occur after trabeculectomy
Pterygium surgery: tends to occur at the conjunctival defect site
Enucleation: 3–7% with implant3)

A conjunctival inclusion cyst is a benign cystic lesion in which conjunctival epithelium becomes entrapped in the substantia propria of the mucosa and forms a cyst wall. The cyst wall is composed of non-keratinized epithelium containing goblet cells, and the lumen contains clear to slightly turbid fluid including keratin, mucin, and epithelial debris.
Conjunctival cysts are classified into the following three types based on the mechanism of formation.
| Classification | Characteristics |
|---|---|
| Inclusion cyst | Due to epithelial entrapment |
| Lymphatic cyst | Lymphangiectasia |
| Retention cyst | Accessory lacrimal gland origin |
Conjunctival cysts account for 3% of all orbital cysts. They are broadly classified into primary (congenital) and secondary (acquired) types. Congenital cysts result from excessive invagination of the caruncular epithelium or fornical conjunctiva during embryonic development.
The average age of onset is around 47 years, with no gender difference. Among conjunctival cysts, inclusion cysts are the most common, accounting for approximately 80%. Only 6 cases of congenital cysts attached to the lateral rectus or inferior rectus muscle have been reported in the literature5).
Conjunctival cysts are mainly classified into three types: ① Conjunctival inclusion cyst: formed by ectopic conjunctival epithelium, most common. ② Lymphatic cyst: caused by dilation of lymphatic vessels. ③ Retention cyst: formed in the fornix due to obstruction of the secretory ducts of accessory lacrimal glands (Wolfring glands, Krause glands). All are benign, but differentiation from malignant tumors may be necessary, so an ophthalmology consultation is recommended.
Small cysts are often asymptomatic. As the cyst enlarges, it rubs against the palpebral conjunctiva during blinking, causing foreign body sensation and tearing. Giant cysts may present with restricted eye movement, diplopia, and proptosis. Some patients seek medical attention for cosmetic concerns. Congenital giant cysts have been detected by prenatal ultrasound7).
Slit-lamp examination reveals a translucent dome-shaped elevation on the bulbar conjunctiva. It is mobile and transilluminable. When epithelial cells deposit at the bottom of the cyst, it may appear as a pseudohypopyon.
Cysts after strabismus surgery commonly occur in the temporal conjunctiva and become apparent 3 to 6 months postoperatively4). Orbital cysts after enucleation are often discovered due to difficulty retaining the prosthesis1)3).
The most common cause is ophthalmic surgery. Cysts form when conjunctival epithelium is inadvertently trapped in the subconjunctival tissue during surgery.
Surgery-related
Strabismus surgery: incidence 0.25–2.3%4)9)
Glaucoma surgery: can occur after trabeculectomy
Pterygium surgery: tends to occur at the conjunctival defect site
Enucleation: 3–7% with implant3)
Non-surgery-related
Trauma: penetrating or blunt ocular surface injury
Inflammation: Stevens-Johnson syndrome (SJS) causes extensive conjunctival inflammation and adhesions in the acute phase2)
Sub-Tenon anesthesia: cyst formation at the injection site
Idiopathic: often of unknown cause
It is thought to be caused by excessive invagination of the caruncular epithelium or fornical conjunctiva during embryogenesis5). Only 4 cases of congenital conjunctival cysts detected by prenatal ultrasound have been reported in the literature7).
Three mechanisms of cyst formation after enucleation have been proposed by McCarthy et al.3): (1) proliferation of conjunctival tissue placed into the orbit during enucleation, (2) invagination of everted conjunctiva after wound closure, and (3) downward epithelial proliferation after implant extrusion.
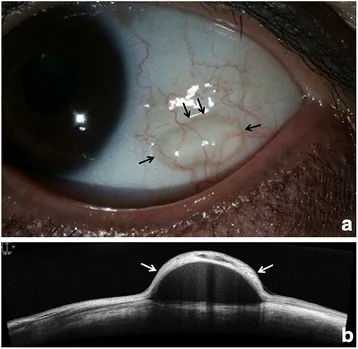
A translucent dome-shaped elevation, good mobility, and transillumination are observed. Fluorescein staining is usually negative.
The cyst lumen is depicted as a hyporeflective area with a thin hyperreflective cyst wall. Scattered granular hyperreflective images within the lumen suggest an inclusion cyst. It is excellent for evaluating small cysts.
The cyst lumen is depicted as a hypoechoic area. Floating particles may be observed in secondary cysts. It is superior to anterior segment OCT in evaluating tumor boundaries and the posterior wall.
Definitive diagnosis is based on pathological findings. The cyst wall is lined with non-keratinized cuboidal to columnar epithelium containing goblet cells, characteristic of conjunctival epithelial inclusion cysts4). Inflammatory or granulomatous changes are usually absent4).
| Differential Diagnosis | Key Differentiating Features |
|---|---|
| Lymphatic Cyst | Multilocular, high translucency |
| Conjunctival Myxoma | Solid, not suitable for aspiration8) |
| Dermoid Cyst | Keratinized epithelium, bone erosion |
Conjunctival myxoma presents a translucent cyst-like appearance and is easily misdiagnosed as a conjunctival inclusion cyst8). Aspiration alone carries a risk of missing the diagnosis, so definitive diagnosis by excisional biopsy is important8). Attention should also be paid to its association with Carney complex8).
Most transparent to translucent conjunctival bulges are benign conjunctival cysts, but differentiation from other diseases such as conjunctival myxoma and dermoid cyst is necessary. In particular, conjunctival myxoma closely resembles a cyst in appearance, so there is a risk of missing it with aspiration alone. If the lesion does not resolve spontaneously or shows a tendency to enlarge, ophthalmologic examination is recommended.
Asymptomatic small cysts can be observed. They may resolve spontaneously, but this is not common.
The standard treatment for symptomatic cysts is complete excision. It is important to remove the cyst en bloc without rupturing the cyst wall; if completely removed, recurrence does not occur. If the cyst wall is adherent to the sclera, sharp dissection is required 4).
A case has been reported of a conjunctival inclusion cyst measuring 10×8 mm that developed after strabismus surgery, which did not respond to topical steroid eye drops for 3 months and was eventually excised. No recurrence was observed at 6 months postoperatively. 4)
TCA Injection Therapy
Agent: Trichloroacetic acid 10–20%
Indications: Recurrent cases, giant cysts
Method: After aspirating the cyst contents, TCA is injected to chemically cauterize the epithelium 6)
Outcomes: Complete resolution and no recurrence at 8 months with 20% TCA 6)
Foam Sclerotherapy
Agent: Sodium tetradecyl sulfate (STS) foam solution
Indications: Orbital cysts after enucleation
Method: After cyst puncture and aspiration, STS foam is injected to induce fibrosis of the cyst wall 1)
Outcomes: Complete resolution at 6 weeks 1)
Marsupialization
Indications: Large cysts (diameter ≥1 cm) associated with Stevens-Johnson syndrome
Method: Reconstruct the ocular surface by reusing the cyst wall as a lining for the conjunctival fornix2)
Outcomes: No recurrence in 4 cases during follow-up of 7 months to 3 years2)
For symptomatic cysts, artificial tears and low-potency steroid eye drops are used. It is rare for cysts to resolve with eye drops alone; if insufficient, surgery is indicated.
Small conjunctival inclusion cysts may resolve spontaneously, but this is not common. If asymptomatic, observation is possible. If symptomatic or enlarging, treatments such as complete excision or TCA injection are considered. Simple aspiration is not recommended due to high recurrence.
When conjunctival epithelium becomes entrapped in the substantia propria due to trauma or surgery, the entrapped epithelium continues to proliferate and forms a cyst cavity. The cyst wall consists of non-keratinized lining epithelium and connective tissue, often containing goblet cells. Mucin secretion by goblet cells contributes to cyst enlargement.
In the acute phase of Stevens-Johnson syndrome, extensive ocular surface inflammation and epithelial necrosis occur2). Acute ocular involvement in Stevens-Johnson syndrome is observed in 77% of patients2). During the scarring and adhesion process after inflammation, residual conjunctival epithelium becomes entrapped, forming large cysts. The cyst wall is histologically similar to conjunctival epithelium and can secrete fluid to moisten the ocular surface2).
Congenital conjunctival cysts result from abnormal invagination of conjunctival epithelium during embryonic development. Pathologically, they are observed as cysts lined by non-keratinized squamous epithelium and focal cuboidal epithelium 7). They may also be classified as a conjunctivoid variant of dermoid tumors 7).
The fourth case of prenatal ultrasound detection of congenital conjunctival cyst was reported in 2025 7). With advances in prenatal imaging, the possibility of early detection and planned surgical intervention is expanding.
In terms of treatment, the application of foam sclerotherapy (STS) to orbital cysts has been reported 1), attracting attention as a new low-cost, simple, and repeatable option. Injection of TCA 20% is also accumulating evidence as an effective alternative treatment for recurrent cases after resection 6).
Marsupialization for cases complicated by Stevens-Johnson syndrome is an innovative technique that utilizes the cyst wall for conjunctival fornix reconstruction 2), and further case accumulation and long-term outcome verification are expected.
In differential diagnosis, the risk of overlooking conjunctival myxoma has been pointed out 8), and the importance of definitive diagnosis by excisional biopsy rather than puncture alone is being reaffirmed for lesions with a cyst-like appearance.