An ocular bee sting is a sting to the eye area by a bee or wasp. Both belong to the order Hymenoptera, but the venom components differ, leading to different clinical presentations 4). Stings to the cornea, conjunctiva, sclera, or eyelid can cause devastating damage to eye health and visual function.
Published data on ocular bee stings are limited, mostly consisting of case reports and small case series. A literature review of 35 reports involving 56 cases found that the cornea was the most common sting site, with conjunctival stings accounting for only about 9% 2). No standardized treatment protocol currently exists 5).
The venom from a single bee is not lethal to humans, but it can cause fatal damage to the eye. Wasps, in particular, have a large amount of venom and a stinger about 7.0 mm long. Stings to the canthus can reach Tenon’s capsule, and stings to the eyeball can reach the anterior chamber, lens, and vitreous body. If there is a history of bee stings, there is a risk of anaphylactic shock regardless of the bee species.
QHow do honeybee and wasp stings differ?
A
Honeybees have barbed stingers that become fixed in tissue, leaving the stinger in the body and causing the bee to die. Wasps have smooth stingers that are not fixed, allowing them to sting multiple times and inject more venom. Wasp stings tend to have more severe outcomes than honeybee stings. Local eyelid reactions are also stronger in the order of honeybees, paper wasps, and wasps.
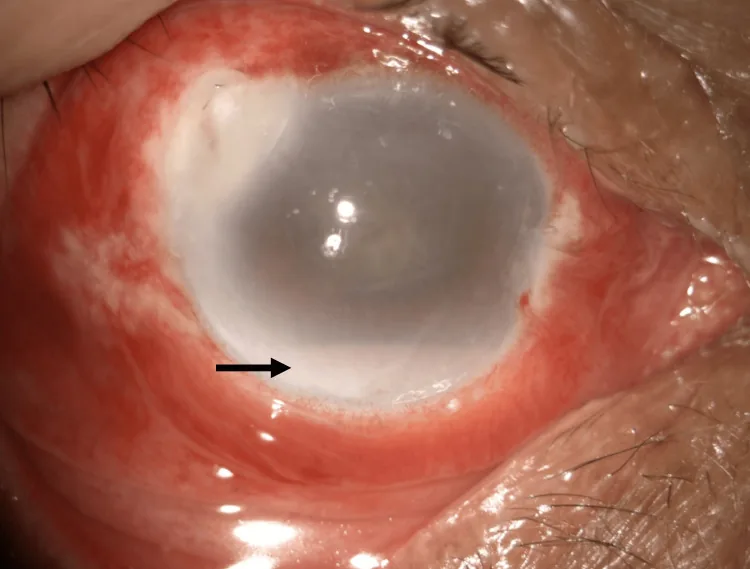
Muhammad Hafiz As-Shaarani Mohd Amin, Abdul-Hadi Rosli, Adzura Salam Ocular Hornet Injury: A Case Report on Corneal Microperforation and Endophthalmitis 2024 Jul 27 Cureus.; 16(7):e65515 Figure 2. PMCID: PMC11346803. License: CC BY.
Anterior segment photograph of the right eye. The black arrow indicates sterile hypopyon suggesting endophthalmitis. Corneal opacity and conjunctival injection are also observed.
Ocular bee stings present a variety of clinical manifestations. A literature review of 56 cases reported anterior chamber inflammation in 59%, cataract in 34%, elevated intraocular pressure in 18%, and optic neuropathy in 2.27% 2).
Toxic Keratopathy
Sterile corneal ulcer: Occurs around the embedded stinger in the deep stroma.
Corneal edema: Accompanied by Descemet’s membrane folds, spreading locally to diffusely.
Residual stinger findings: Characteristic finding of a “fine raised network” on the epithelium.
Endothelial damage: Decreased cell density and pleomorphism may occur long-term.
Optic neuritis: Develops hours to days after injury. Visual acuity may decrease to light perception.
Segmental iris atrophy: Due to direct toxic damage.
Glaucoma: Short-term and long-term elevation of intraocular pressure.
Even a spray of hornet venom alone can cause severe corneal damage as a chemical injury. Venom that infiltrates the eye continuously destroys intraocular tissues.
Bee venom contains amines that cause pain and swelling, pain-inducing peptides that cause intense pain, membrane-active peptides that act on cell membranes, hydrolytic enzymes that cause tissue destruction, and high-molecular-weight proteins that act as antigens.
There are no established risk factors for poor prognosis after ocular bee sting. The anatomical site of the sting, depth of the retained stinger, type of bee, and timing of treatment intervention are thought to affect prognosis.
Detailed history taking: Confirm the type of bee, time of injury, sting site, and duration the bee was on the skin. Also note the presence of systemic symptoms.
Slit-lamp examination: Evaluate for retained stinger, corneal edema, hypopyon, corneal leukoma, iris atrophy, etc.
Fundus examination: Check for optic disc edema.
B-mode ultrasonography: If the posterior pole is not visible, rule out vitritis or retinal detachment.
Even if the eyelid is stung rather than the eyeball, use slit-lamp microscopy to check for ocular injury. Examination is necessary even if the bee only flew in front of the eye.
Any disease that causes corneal opacity, corneal edema, conjunctival injection, or intraocular inflammation should be considered. Confirming exposure history is most important. Differential diagnoses include infectious keratitis, herpetic stromal keratitis, Fuchs endothelial corneal dystrophy, and corneal ulcers due to autoimmune diseases.
Immediately after injury, remove the stinger promptly to limit venom injection 3). Honeybees leave the stinger with the venom sac attached; grasp the base of the stinger with forceps and remove it without crushing the sac. Approximately 90% of honeybee venom is injected within 30 seconds of the sting.
If time has passed since the sting, the venom has already been released, so treat the stinger as a foreign body and remove it as completely as possible. Examination under slit-lamp microscopy to identify all fragments is recommended. Early stinger removal and topical pharmacotherapy have been reported to preserve good visual acuity3).
Topical antibiotics: Prevention of secondary infection
Topical steroids: Suppression of inflammatory secondary damage. Frequent instillation is recommended
Topical cycloplegics: Added when there is anterior chamber inflammation
Oral steroids: Considered effective for improving final visual acuity and preventing optic neuritis. In a case series of 11 eyes, oral steroids were used in 5 of 6 eyes that achieved good outcomes with medical treatment alone, and may contribute to preventing vision-threatening complications such as corneal endothelial decompensation, cataract, and glaucoma1)
Subconjunctival steroid injection: In cases of globe penetration, it is more effective intraocularly than drops or systemic administration
It has been reported that prompt removal of the stinger and high-dose topical and systemic steroid administration can suppress permanent corneal damage and intraocular complications4). On the other hand, it is also pointed out that surgical intervention after excluding infectious conditions and careful steroid use affect prognosis, and there are cases that followed a favorable course with conservative treatment5).
Hornet venom spray is treated as a chemical injury. Since there is no antidote, the only method is physical dilution. Anterior chamber irrigation with intraocular irrigation solution should be performed as soon as possible. The time from injury to treatment determines the prognosis.
Apply steroid eye ointment and antibiotic eye ointment several times a day. Apply cold compresses and maintain local rest. If inflammation is severe, add oral antihistamines or steroids. Local eyelid reactions are strongest with honeybees, followed by paper wasps, then hornets. With hornets, ulcers may form and healing may take more than one month.
If within 30 seconds of injury, the stinger should be removed immediately to prevent further venom injection. After that, venom has already been released, so the stinger is treated as a foreign body. Although some cases have had uneventful outcomes with long-term retention, complete removal is recommended if possible.
The injury mechanism of ocular bee sting is understood as a trauma triad combining penetrating injury from the stinger, immune reaction to bee venom components, and toxic damage from the venom itself 3). Membrane-active peptides in bee venom (e.g., melittin) directly destroy cell membranes of corneal epithelium, stroma, and endothelium. Phospholipase A2 degrades phospholipids and induces cell death. Hyaluronidase acts as a tissue spreading factor, promoting venom penetration.
The corneal endothelium is particularly vulnerable to toxins, with long-term persistence of decreased cell density and pleomorphism. Irreversible damage to endothelial cells can cause delayed corneal edema.
Two mechanisms are hypothesized for optic neuritis after a sting.
Direct toxicity: The toxin penetrates the vitreous cavity, reaches the posterior segment, and damages the optic nerve.
Immunological mechanism: Some cases develop bilateral optic neuritis after a unilateral sting, suggesting involvement of an immune response to bee venom components.
Bee venom contains high-molecular-weight proteins, and in individuals with a history of bee stings, there is a risk of IgE-mediated anaphylactic shock. Monitoring of systemic condition is essential alongside management of ocular symptoms.
Prognosis depends on the sting site, depth of retained stinger, bee species, and timeliness of therapeutic intervention. Visual outcomes range from 20/20 to light perception. In a case series of 11 eyes by Gudiseva et al., 54.5% had good outcomes with medical treatment alone, while the remaining 45.5% required surgical interventions such as corneal transplantation or cataract surgery. Among the 5 surgical eyes, 3 developed glaucoma, and 1 required trabeculectomy1).
Prompt initiation of appropriate treatment often leads to favorable outcomes. Conversely, hornet stings, optic neuritis, and delayed treatment are poor prognostic factors. If corneal opacity, cataract, or glaucoma persists, surgical intervention for visual recovery is considered.
Gudiseva H, Uddaraju M, Pradhan S, Das M, Mascarenhas J, Srinivasan M, Prajna NV. Ocular manifestations of isolated corneal bee sting injury, management strategies, and clinical outcomes. Indian J Ophthalmol. 2018;66(2):262-268. PMID: 29380771. PMCID: PMC5819108.
Semler-Collery A, Hayek G, Ramadier S, Perone JM. A Case of Conjunctival Bee Sting Injury with Review of the Literature on Ocular Bee Stings. Am J Case Rep. 2019;20:1284-1289. PMID: 31471535. PMCID: PMC6735618.
Lin PH, Wang NK, Hwang YS, Ma DH, Yeh LK. Bee sting of the cornea and conjunctiva: management and outcomes. Cornea. 2011;30(4):392-394. PMID: 21099408.
Siddharthan KS, Raghavan A, Revathi R. Clinical features and management of ocular lesions after stings by hymenopteran insects. Indian J Ophthalmol. 2014;62(2):248-251. PMID: 24618493. PMCID: PMC4005246.