Neurotrophic keratitis (NK) is a degenerative corneal disease characterized by reduced or absent corneal sensation. It is also called neurotrophic keratopathy or neuroparalytic keratopathy. It develops due to impaired sensory innervation from the ophthalmic branch (V1) of the trigeminal nerve (cranial nerve V).
Corneal nerve terminals contain many neurotransmitters such as substance P, calcitonin gene-related peptide (CGRP), neuropeptide Y (NPY), vasoactive intestinal peptide (VIP), galanin, methionine-enkephalin, catecholamines, and acetylcholine. These nerve-derived factors regulate corneal epithelial metabolism, turnover, and wound healing. Reduced supply of these factors due to trigeminal nerve damage is the essential mechanism of corneal homeostasis disruption.
The clinical course progresses in stages. Partial or complete loss of corneal sensation begins with epithelial keratopathy (superficial punctate keratopathy, SPK) and can progress to persistent epithelial defect (PED), corneal stromal ulcer, and even corneal perforation 5). However, if managed appropriately in the early stages, progression can be halted.
The estimated prevalence is less than 50 per 100,000, classifying it as a rare disease 11). The ICD-10 code is H16.239. This disease is not a single entity but rather a syndrome that can result from any condition damaging the trigeminal nerve pathway.
QAre neurotrophic keratitis and neuroparalytic keratopathy the same disease?
A
Neurotrophic keratitis, neurotrophic keratopathy, and neuroparalytic keratopathy all refer to the same condition caused by trigeminal nerve damage. The terms differ in emphasis on whether the corneal epithelial damage is inflammatory or degenerative, but they are clinically equivalent.
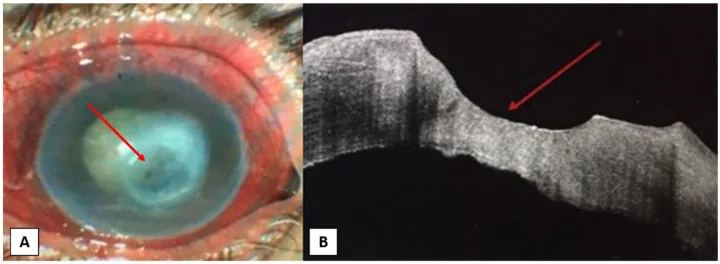
Inferrera L, Aragona E, Wylęgała A, et al. The Role of Hi-Tech Devices in Assessment of Corneal Healing in Patients with Neurotrophic Keratopathy. J Clin Med. 2022;11(6):1602. Figure 1. PMID: 35329927; PMCID: PMC8955972; DOI: 10.3390/jcm11061602. License: CC BY 4.0.
Fluorescein staining image of a patient with post-herpetic neurotrophic keratitis. Shows a large oval persistent corneal epithelial defect with raised edges before treatment (i), and reduction after 4 weeks (ii) and 8 weeks (iii). Corresponds to Mackie grade II persistent epithelial defect (PED) discussed in the section “2. Main Symptoms and Clinical Findings”.
In NK, because corneal sensory innervation is impaired, patients rarely complain of ocular surface symptoms. Therefore, some cases are not seen until several months to years after onset.
Blurred vision and decreased visual acuity: Visual impairment due to punctate keratopathy, epithelial defect, corneal scarring, and edema
Asymptomatic: Lack of pain or foreign body sensation, so patients are unaware until the condition becomes severe
Conjunctival injection and discharge: Mild redness or discharge may be present
In infants: Blinking only in response to threat, or corneal damage from self-injury may be clues
Cases with facial nerve palsy: Incomplete eyelid closure (lagophthalmos) may complicate the clinical picture
The clinical presentation of NK ranges from subtle corneal surface irregularity to corneal melting and perforation. Classically, Mackie’s three-stage classification is widely used 12,13).
Grade I (Mild)
Punctate keratopathy: Mainly punctate irregularities of the corneal epithelium without epithelial defect.
Qualitative epithelial abnormality: Corneal epithelial opacity and decreased transparency.
Tear film instability: May be accompanied by decreased tear secretion and reduced goblet cell density.
Grade II (Moderate)
Persistent epithelial defect (PED): Characterized by an oval shape with rolled margins. May be accompanied by opacification and neovascularization.
Descemet’s membrane folds: A finding associated with corneal edema.
Mild anterior chamber inflammation: Mild inflammation (cell/flare) in the anterior chamber may be observed.
Grade III (Severe)
Corneal stromal ulcer: Stromal defect with corneal melting.
Corneal perforation: The most severe complication. Requires urgent surgical intervention.
Corneal scarring: May cause permanent visual impairment even after healing.
Decreased tear secretion is often a nearly obligatory accompanying finding in NK. During evaluation, Schirmer’s test and tear break-up time (BUT) should always be used in addition to corneal findings 11).
QWhy does it become severe even without symptoms?
A
In NK, damage to the trigeminal nerve reduces or eliminates corneal sensation. Normally, corneal epithelial damage is perceived as pain or a foreign body sensation, but in NK this warning signal does not function. Furthermore, reflex tear secretion and blinking are also reduced, so epithelial defects and ulcers progress without subjective symptoms, leading to delayed consultation and severe disease.
Any ocular or systemic disease that damages the sensory nerve pathway from the cornea to the trigeminal nucleus in the pons can cause NK. From a pathophysiological perspective, causes are broadly classified into peripheral (corneal local to orbital), central (intracranial), and metabolic (diabetes) 13).
Refractive surgery: LASIK significantly more likely than PRK to cause temporary nerve damage due to extensive severing of the subbasal nerve plexus during flap creation.
In diabetic patients, morphological and functional changes in corneal sensory nerves progress, and corneal sensitivity decreases in correlation with the severity of diabetic retinopathy. This is an aspect of diabetic peripheral neuropathy and is considered similar to refractory skin ulcers or diabetic foot gangrene. Cases where NK is discovered as the first sign of diabetes have also been reported 11).
QIs it possible to develop neurotrophic keratitis after LASIK?
A
In LASIK, corneal nerves are cut during flap creation, causing temporary corneal hypoesthesia after surgery. In most cases, it recovers within a few months to a year, but rarely it persists and leads to neurotrophic keratitis. PRK does not create a flap, so the incidence of nerve damage is lower. In cases with pre-existing dry eye or corneal hypoesthesia, careful evaluation is required when selecting the surgical procedure.
This is the most important test for diagnosing NK.
Cochet-Bonnet esthesiometer: Standard contact quantitative evaluation method. A 0.12 mm nylon filament is extended to 60 mm and touched to the cornea of a seated patient. If the patient does not feel it, the filament is shortened by 5 mm. The shortest length at which the patient feels contact is measured three times, and the average is expressed as the filament length (mm). Normal values are 50–60 mm; 45 mm or less indicates reduced corneal sensitivity, and less than 40 mm indicates clear hypoesthesia 1). The central cornea is most sensitive, and sensitivity decreases toward the periphery, so measurements should always be taken at the same site.
Cotton swab test: Qualitative evaluation by touching with a cotton wisp. Simple but poorly reproducible; used for screening.
CRCERT-Belmonte non-contact esthesiometer: Non-contact measurement using air stimulation. Can detect subtle sensitivity changes that are difficult to evaluate with the Cochet-Bonnet esthesiometer 13).
Eye drops (especially anesthetics or preservative-containing drops) alter the measurement values, so sensitivity testing should be performed before instillation.
In vivo confocal microscopy (IVCM): Directly visualizes the structure of the subbasal corneal nerve plexus. In NK, decreased nerve density and abnormal nerve morphology are quantitatively demonstrated 1,10). Useful for evaluating treatment efficacy and follow-up.
Anterior segment OCT: Measures the thickness of epithelial defects and the degree of stromal melting.
When severe corneal epithelial damage is present despite no ocular discomfort due to corneal anesthesia, NK is strongly suspected. Differentiation from the following diseases is necessary.
Dry eye: May be accompanied by some degree of corneal hypoesthesia, but usually patients experience foreign body sensation or eye pain.
Toxic keratopathy from eye drops: Differentiated by medication history.
Active herpetic keratitis: Reduces corneal sensation, but NK is sterile, which is a key difference.
Infectious corneal ulcer: Differentiated by infiltrative findings at the ulcer margin and anterior chamber inflammation.
After diagnosis, investigation of the underlying cause is essential. Obtain history (herpes, diabetes, ocular surgery, trauma, intracranial lesions, eye drops) through interview, and perform head MRI or consult neurology/neurosurgery as needed.
Treatment of NK is based on stage-specific management. Throughout all stages, use preservative-free eye drops. If other ocular surface diseases (dry eye, blepharitis, exposure keratopathy, etc.) are present, treat them concurrently. Also treat the underlying cause.
Aims to protect the epithelium and stabilize the tear film.
Preservative-free artificial tears and lubricating ointments: Frequent instillation (e.g., 0.1% sodium hyaluronate eye drops 5–6 times daily, adjusted as needed) is the mainstay.
Eye ointment: Apply 0.3% ofloxacin eye ointment 2–3 times daily to protect the corneal epithelium.
Rebamipide suspension eye drops (2%): Instill 4 times daily, expecting epithelial protection through mucin secretion promotion.
Punctal occlusion: Insert punctal plugs to promote tear retention when tear secretion is significantly reduced.
Autologous serum eye drops: Consider for persistent corneal epitheliopathy. Promotes wound healing by supplying growth factors (EGF, FGF, TGF-β).
Treatment of Grade II (Persistent Epithelial Defect)
In addition to treatment for Grade I, the following are used.
Therapeutic soft contact lens (TCL): Protects the cornea as a bandage lens and promotes epithelial healing
Amniotic membrane transplantation (AMT): Covers and protects the fragile corneal epithelium, promotes epithelial regeneration through anti-inflammatory and anti-scarring effects and supply of basement membrane components. Corneal epithelial extension is observed with fluorescein staining, and the membrane is removed after re-epithelialization is confirmed
Tarsorrhaphy (temporary/permanent): Reduces mechanical irritation and improves tear retention. Partial tarsorrhaphy is effective in severe cases
Botulinum toxin injection: Induces ptosis by paralyzing the levator muscle as an alternative to tarsorrhaphy, promoting eyelid closure
Antibiotic eye drops: Prevention of secondary infection
Cenegermin (Oxervate™): Recombinant human nerve growth factor (rhNGF) 20 μg/mL eye drops. Approved as the first drug for stage II and III NK by the European Medicines Agency (EMA, 2017) and the U.S. Food and Drug Administration (FDA, 2018)2). Dosage: 6 times daily for 8 weeks2)
In clinical trials of cenegermin, a randomized vehicle-controlled double-blind study (REPARO phase II, Pflugfelder 2020 pivotal trial) was conducted in patients with stage II or III NK8,9).
Pooling two randomized controlled trials, 65–72% of patients in the rhNGF eye drop group achieved complete corneal healing after 8 weeks, compared to 17–33% in the vehicle control group. The most common adverse event was instillation site pain, occurring in about 16% of patients3).
The REPARO phase I/II trial (NGF0212) showed reduced epithelial defect healing time and lower recurrence rates, but did not demonstrate significant improvement in corneal sensation itself2). Some patients experience recurrence of NK after treatment discontinuation, requiring regular follow-up.
Topical steroids should be used cautiously for inflammation control as they may induce stromal melting. Topical NSAIDs should be avoided as they further reduce corneal sensation. Continuous use of topical anesthetics is strictly contraindicated.
In Japan, the following treatments that promote corneal epithelial wound healing have been reported at the clinical research level. For cases unresponsive to standard treatment, consultation with facilities capable of performing these treatments may be considered.
Substance P + insulin-like growth factor-1 (IGF-1) combination eye drops: The combination of the essential minimal sequences FGLM-NH₂ and SSSR has been reported to promote epithelial wound healing
Fibronectin eye drops: Promote cell adhesion and assist epithelial extension
Nerve growth factor (NGF) eye drops: Act directly on corneal epithelial cells (in Japan, studied in a different formulation from cenegermin)
Umbilical cord serum eye drops: Rich in growth factors similar to autologous serum, used in cases where autologous blood collection is difficult
Corneal neurotization (CN): A radical surgical treatment that transfers healthy sensory nerves to the peripheral cornea to restore corneal innervation itself1,4)
Corneal nerve regeneration has traditionally been indicated for severe cases unresponsive to conservative treatment, but with recent advances in minimally invasive techniques, the indications are expanding 1). Candidates include patients with moderate to severe corneal hypoesthesia or anesthesia resistant to conservative treatment, who have healthy donor nerves available 4). Donor nerves include trigeminal branches (supraorbital, supratrochlear, infraorbital) and the great auricular nerve (GAN) from the neck 1).
The axon counts of donor nerves are reported as follows: GAN average 6,530; supraorbital nerve approximately 3,146 (distally, about 6,000 at the orbital rim); supratrochlear nerve 1,882 (distally, 2,534 at the orbital rim); sural nerve 3,179–3,972 1). It is believed that a higher axon count leads to better nerve regeneration.
Surgical techniques are broadly classified into direct neurotization and indirect nerve grafting 1,7).
Direct method: The donor nerve is mobilized and its end is directly transplanted to the corneal periphery. Since continuity is preserved, sensory recovery is faster, but the reach of the donor nerve is limited.
Indirect method: An autologous nerve (e.g., sural or great auricular nerve) or an acellular allogeneic nerve allograft (Axogen, up to 70 mm) is used as an interposition graft to connect the donor nerve to the cornea. Surgery time is shorter, but recovery takes longer because axons must pass through the graft.
Anastomosis methods include end-to-end (complete transection of the donor nerve to maximize axon load) and end-to-side (creating a window in the donor nerve sheath to preserve residual function); the latter can reduce sensory loss in the donor area 1). A prospective multicenter comparative trial found no significant difference in Cochet-Bonnet improvement at 12 months between direct and indirect methods 7).
The donor nerve reaching the cornea is divided into 3–4 fascicles, which are inserted into scleral-corneal tunnels around the limbus or fixed to the limbus with fibrin glue or sutures 1). Postoperatively, a bandage contact lens and temporary tarsorrhaphy are used for protection, along with preservative-free artificial tears and antibacterial eye drops. Starting one month after surgery, adjunctive use of cenegermin eye drops is expected to promote corneal nerve growth 1).
QWhat kind of drug is cenegermin (Oxervate)?
A
Cenegermin is an eye drop containing 20 μg/mL of recombinant human nerve growth factor (rhNGF) and is the first approved treatment for NK. In clinical trials for stage II and III NK (REPARO phase II, pivotal phase II), instillation 6 times daily for 8 weeks resulted in complete corneal healing in 65–72% of patients. However, it has not been shown to significantly improve corneal sensation itself, and there are cases of recurrence after discontinuation. The main side effect is instillation site pain (approximately 16%).
QWhat is corneal nerve regeneration surgery?
A
Corneal nerve regeneration surgery is a procedure that transfers healthy sensory nerves (such as the supraorbital, supratrochlear, infraorbital, and great auricular nerves) to the peripheral cornea to restore sensation in neurotrophic corneas. There are direct nerve transfer methods and indirect nerve graft methods using the sural nerve. Corneal sensation recovery begins 3–6 months after surgery and continues to improve over 12–18 months or more. In a review of 54 eyes by Park et al., the mean Cochet-Bonnet value recovered from 2.18 mm to 40.1 mm. Younger patients under 18 years tend to have better recovery.
The cornea is one of the most densely innervated tissues in the human body. The long ciliary nerves, branching from the first division of the trigeminal nerve (ophthalmic nerve), reach the cornea. Nerve fibers enter the corneal stroma radially from the limbus and form the sub-epithelial plexus just below Bowman’s layer. They then penetrate Bowman’s layer to form the sub-basal nerve plexus and extend free nerve endings between epithelial cells. The nerve fibers are unmyelinated, consisting of thin Aδ and C fibers, contributing to corneal transparency.
This sub-basal nerve plexus supplies neurotrophic factors essential for maintaining corneal epithelial homeostasis 1,8). Nerve fibers contain substance P, which enhances the effects of epidermal growth factor (EGF) and insulin-like growth factor-1 (IGF-1) on corneal epithelial cell migration, thereby regulating epithelial wound healing. When the trigeminal nerve is damaged, this regulatory mechanism is lost, and reflex tear secretion and blinking are also reduced, leading to a state where corneal epithelial damage progresses easily and healing is delayed.
Decreased goblet cell density: reduced secretory function of the conjunctiva
Animal models have shown that healing of artificial corneal epithelial defects is significantly delayed in rats with trigeminal nerve destruction compared to control groups, experimentally confirming that loss of neural factors is a central mechanism of delayed wound healing.
NGF is a representative molecule of the neurotrophin family and becomes active after cleavage from its precursor pro-NGF. The active form is a β-NGF dimer (molecular weight 26 kDa), composed of two non-covalently linked β subunits2).
NGF binds to the following two receptors2):
TrkA^NGFR^: high-affinity receptor. Activation drives downstream signaling via the MAPK, PI3K, and PLC pathways
p75^NTR^: low-affinity receptor. Plays an auxiliary role
These receptors are constitutively expressed on corneal epithelial cells and conjunctival basal epithelial cells. NGF promotes proliferation and differentiation of corneal epithelial cells and contributes to wound healing2). In NK patients, NGF supply is reduced, contributing to disruption of epithelial homeostasis. The clinical efficacy of rhNGF eye drops in the REPARO trial is positioned as a disease-specific treatment based on this molecular mechanism8,9).
Decreased corneal sensitivity in diabetic patients is considered a phenotype of diabetic peripheral neuropathy. It is known that corneal sensitivity decreases in correlation with the severity of diabetic retinopathy, and morphological changes in corneal nerves progress in correlation with renal function decline. This is an ocular surface manifestation of peripheral sensory neuropathy similar to diabetic foot gangrene and refractory skin ulcers, and is an important pathological basis of neurotrophic keratopathy13).
Nerve Regeneration Mechanism of Corneal Neurotization
In corneal neurotization, after transferring a healthy sensory nerve to the corneal periphery, axonal regeneration proceeds following the process of Wallerian degeneration1).
Initial injury response: Axons at the distal end of the donor nerve degenerate, and macrophages phagocytose and remove the degenerated myelin.
Schwann cell guidance: Schwann cells differentiate and migrate from the viable proximal end of the donor nerve, providing a scaffold for axonal regeneration.
Axonal sprouting: NGF and interleukin-1 (IL-1) promote axonal sprouting 1).
Selective regeneration: The cornea selectively accepts only unmyelinated nerves of a specific phenotype, so only a portion of regenerating axons reach the corneal stroma and subbasal nerve plexus 1).
Interestingly, animal studies have shown that regenerated corneal nerves are not necessarily continuous with the donor nerve, suggesting that the donor nerve may function not only as a source of axons but also as a source of neurotrophic factors 1).
7. Latest Research and Future Perspectives (Investigational Reports)
Corneal neurotization has evolved from a large-scale procedure requiring a coronal incision to minimally invasive approaches and endoscopic techniques 1,14). The introduction of acellular allogeneic nerve allografts has made it possible to avoid complications associated with autologous nerve harvesting, and the use of alternative donor nerves (e.g., great auricular nerve) has expanded indications 1).
In terms of outcomes, a review of 54 eyes by Park et al. reported that the Cochet-Bonnet value recovered from a preoperative mean of 2.18 mm to a postoperative mean of 40.1 mm 1,6). Younger patients under 18 years of age tend to achieve earlier and more complete sensory recovery and visual improvement, which is thought to be due to higher subbasal nerve fiber density in younger individuals 1,6). Visualization of corneal nerves by in vivo confocal microscopy begins at 3 months postoperatively and continues to improve over 12 to 18 months 1,14). After stabilization of the ocular surface by corneal neurotization, staged visual rehabilitation with penetrating keratoplasty (PK) or deep anterior lamellar keratoplasty (DALK) has been performed with good outcomes 1).
Since receiving FDA/EMA approval, real-world clinical data on cenegermin have been accumulating. Recently, a phase II trial for dry eye syndrome reported improvements in symptoms, ocular surface staining, and tear secretion 2). Its application to other ocular surface diseases is also being considered.
Thymosin β4 0.1% ophthalmic solution (RGN-259) demonstrated promotion of corneal healing and improvement of subjective symptoms in a randomized, placebo-controlled, double-blind phase III clinical trial in patients with neurotrophic keratopathy3).
Thymosin β4 is an actin-binding protein that is thought to promote epithelial repair through cell migration, anti-inflammatory, and anti-apoptotic effects 15).
Topical insulin, which has been reported for use in corneal diseases since 1945, promotes re-epithelialization of the corneal epithelium. Insulin receptors and IGF-1 receptors have been confirmed to be expressed on the human ocular surface. Although a consensus on dosage has not been established, it is generally administered four times daily. Due to its low cost and high availability, it is expected to be useful in a wide range of regions, including developing countries.
Topically administered RGTA (regenerating agent) is a heparan sulfate proteoglycan mimetic, and observational studies have reported promotion of corneal healing. It is currently only available in Europe.
Substance P/IGF-1 combination as advanced medical treatment
In Japan, research on eye drops containing a combination of neuropeptides that directly act on corneal epithelial cells is ongoing. The combination of the minimal essential sequences FGLM-NH₂ (derived from substance P) and SSSR (derived from IGF-1) has been shown to promote epithelial wound healing, and its application to refractory cases is expected.
Hubschman S, Rosenblatt MI, Cortina MS. Corneal neurotization for the treatment of neurotrophic keratopathy. Curr Opin Ophthalmol. 2025;36(4):294-300. doi:10.1097/icu.0000000000001138.
Levi N Kanu, Joseph B Ciolino. Nerve Growth Factor as an Ocular Therapy: Applications, Challenges, and Future Directions. Seminars in Ophthalmology. 2021;36(4):224-231. doi:10.1080/08820538.2021.1890793.
TFOS DEWS III Management and Therapy Subcommittee. TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;279:355-440.
Dragnea DC, Krolo I, Koppen C, et al. Corneal neurotization-indications, surgical techniques and outcomes. J Clin Med. 2023;12:2214. doi:10.3390/jcm12062214.
Neurotrophic Keratopathy Study Group. Neurotrophic keratopathy: An updated understanding. The ocular surface. 2023;30:129-138. doi:10.1016/j.jtos.2023.09.001. PMID:37666470.
Park JK, Charlson ES, Leyngold I, Kossler AL. Corneal Neurotization: A Review of Pathophysiology and Outcomes. Ophthalmic plastic and reconstructive surgery. 2020;36(5):431-437. doi:10.1097/IOP.0000000000001583. PMID:31923091.
Fogagnolo P, Giannaccare G, Bolognesi F, Digiuni M, Tranchina L, Rossetti L, et al. Direct Versus Indirect Corneal Neurotization for the Treatment of Neurotrophic Keratopathy: A Multicenter Prospective Comparative Study. American journal of ophthalmology. 2020;220:203-214. doi:10.1016/j.ajo.2020.07.003. PMID:32659280.
Bonini S, Lambiase A, Rama P, Sinigaglia F, Allegretti M, Chao W, et al. Phase II Randomized, Double-Masked, Vehicle-Controlled Trial of Recombinant Human Nerve Growth Factor for Neurotrophic Keratitis. Ophthalmology. 2018;125(9):1332-1343. doi:10.1016/j.ophtha.2018.02.022. PMID:29653858.
Pflugfelder SC, Massaro-Giordano M, Perez VL, Hamrah P, Deng SX, Espandar L, et al. Topical Recombinant Human Nerve Growth Factor (Cenegermin) for Neurotrophic Keratopathy: A Multicenter Randomized Vehicle-Controlled Pivotal Trial. Ophthalmology. 2020;127(1):14-26. doi:10.1016/j.ophtha.2019.08.020. PMID:31585826.
Mastropasqua L, Nubile M, Lanzini M, et al. Corneal subbasal nerve plexus changes in patients with neurotrophic keratitis: an in vivo confocal microscopy study. Clin Ther. 2020;42(2):291-302.
Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014;8:571-579. doi:10.2147/opth.s45921.
Ruiz-Lozano RE, Hernandez-Camarena JC, Loya-Garcia D, Merayo-Lloves J, Rodriguez-Garcia A. The molecular basis of neurotrophic keratopathy: Diagnostic and therapeutic implications. A review. The ocular surface. 2021;19:224-240. doi:10.1016/j.jtos.2020.09.007. PMID:33022412.
Dua HS, Said DG, Messmer EM, et al. Neurotrophic keratopathy. Prog Retin Eye Res. 2018;66:107-131. doi:10.1016/j.preteyeres.2018.04.003. PMID:29698813.
Catapano J, Fung SSM, Halliday W, Jobst C, Cheyne D, Ho ES, et al. Treatment of neurotrophic keratopathy with minimally invasive corneal neurotisation: long-term clinical outcomes and evidence of corneal reinnervation. The British journal of ophthalmology. 2019;103(12):1724-1731. doi:10.1136/bjophthalmol-2018-313042. PMID:30770356.
Sosne G, Kleinman HK. Primary Mechanisms of Thymosin β4 Repair Activity in Dry Eye Disorders and Other Tissue Injuries. Investigative ophthalmology & visual science. 2015;56(9):5110-7. doi:10.1167/iovs.15-16890. PMID:26241398.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.