Oxervate™ is an ophthalmic solution containing 0.002% (20 μg/mL) cenegermin-bkbj as the active ingredient. It is a recombinant human nerve growth factor (rhNGF) produced using Escherichia coli.
In August 2018, it was approved by the U.S. Food and Drug Administration (FDA) for the treatment of neurotrophic keratitis (NK). It is the first and only FDA-approved treatment for NK, and also the first topical ophthalmic biopharmaceutical. The European Medicines Agency (EMA) approved it in July 2017 for Mackie classification Stage 2-3 NK in patients aged 18 years and older2).
Nerve growth factor (NGF) is a type of neurotrophin discovered by Rita Levi-Montalcini in the 1950s 4). It has been shown to be essential for corneal and conjunctival nutrition, sensory maintenance, and wound healing. In the late 1990s, a pilot study of topical NGF administration in NK patients was conducted, confirming its safety 4). Subsequently, after a Phase I trial in 2013, efficacy was demonstrated in Phase II (REPARO) and Phase III (NGF0214) trials, leading to approval.
NK is a rare disease (orphan disease) with a prevalence of 1–5 per 10,000 2), and NK is implicated in 13–27% of corneal ulcer patients 3).
QIs Oxervate available in Japan?
A
As of 2025, Oxervate is not approved in Japan. In Japan, symptomatic treatments such as artificial tears, ointments, therapeutic contact lenses, and amniotic membrane transplantation are the mainstay for NK. Some medical institutions also offer clinical research-level treatments such as combined substance P and IGF-1 eye drops.
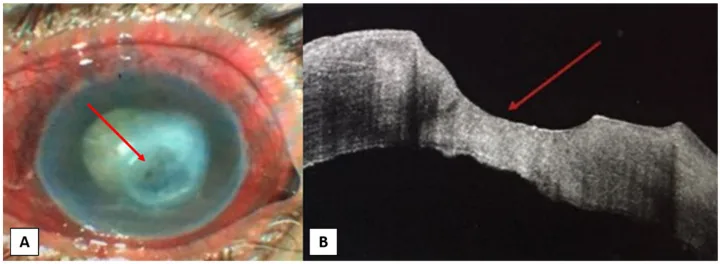
Ahmed A Abdelghany, Francesco D’Oria, Jorge Alio Del Barrio, Jorge L Alio The Value of Anterior Segment Optical Coherence Tomography in Different Types of Corneal Infections: An Update 2021 Jun 27 J Clin Med. 2021 Jun 27; 10(13):2841 Figure 1. PMCID: PMC8267702. License: CC BY.
A: Clinical photograph showing corneal ulcer (indicated by red arrow) and opacity in the patient’s eye. B: AS-OCT image showing corneal epithelial defect at the ulcer site (indicated by red arrow), corneal stromal thinning, and irregular corneal endothelium.
This section outlines the symptoms and findings of neurotrophic keratitis (NK), the indicated disease for oxerbet.
The most characteristic feature of NK is that patients do not perceive pain due to decreased corneal sensation. The lack of subjective symptoms compared to objective corneal findings makes diagnosis difficult.
Decreased visual acuity: Noticed when epithelial damage extends to the visual axis.
Hyperemia: May be accompanied by conjunctival injection
Foreign body sensation: May be felt as mild discomfort
Tear film abnormality: Decreased tear secretion or shortened tear break-up time (BUT).
Corneal hypoesthesia: Decreased corneal sensation in one or more quadrants.
Stage 2 (Moderate)
Persistent epithelial defect: Epithelial defect persisting for more than 2 weeks. Accompanied by marginal opacity and elevation.
Corneal edema and opacity: Stromal changes around the epithelial defect.
Stage 3 (Severe)
Corneal ulcer: Deep stromal involvement with melting.
Perforation risk: Progressive thinning may lead to perforation.
Sterile hypopyon: Rarely appears 1).
Zambino et al. (2021) reported a case of Stage 3 NK after herpes zoster keratitis with sterile hypopyon (1.6 mm). Corneal cultures were negative three times, and cenegermin monotherapy was initiated without corticosteroids. The hypopyon resolved within 4 weeks, and epithelial closure was achieved at 8 weeks 1).
Corneal transplantation, cataract surgery, refractive surgery
Radiation exposure: Develops after orbital radiotherapy. Cases have been reported following radiation for orbital metastasis of breast cancer and pediatric radiation for rhabdomyosarcoma2)
Diabetes: The severity of diabetic retinopathy correlates with decreased corneal sensitivity. Diabetic keratopathy also has aspects of neurotrophic keratopathy.
Chemical trauma / chronic use of eye drops: Long-term exposure to preservatives (benzalkonium chloride) can damage corneal nerves.
Detection of reduced corneal sensitivity is essential for diagnosing NK.
Cochet-Bonnet esthesiometer: The most widely used quantitative test. It adjusts pressure on the corneal surface by varying the length of a nylon filament. A length of less than 40 mm indicates reduced sensation. Sensitivity is highest at the center and decreases toward the periphery.
Gauze method (simple method): A semi-quantitative assessment using the tip of sterile gauze on a scale of 0 to 3 3). Useful in children or when cooperation is difficult.
Cotton swab method: A simple screening method in which the tip of a cotton swab is touched to the cornea and the response is observed.
It is important to differentiate from other diseases that present with epithelial defects. Corneal infections (such as Acanthamoeba keratitis) are ruled out by culture testing 1). For differentiation from exposure keratopathy, drug-induced corneal epithelial disorders, and limbal stem cell deficiency, a combination of history taking regarding exposure and eye drop use, along with corneal sensitivity testing, is useful.
Symptomatic treatment aimed at protecting the epithelium is performed.
Artificial tears and hyaluronic acid eye drops: Use preservative-free preparations. If tear secretion is reduced, instill hyaluronic acid 0.1% 5–6 times daily.
Substance P + IGF-1 combination eye drops: A combination of minimal essential peptides (FGLM-NH₂+SSSR) with corneal epithelial wound healing effects is used at the clinical research level.
Tarsorrhaphy: Considered when forced eyelid closure does not improve the condition
Corneal neurotization: A surgical procedure that transplants healthy sensory nerves to the corneal limbus to promote corneal reinnervation. Indicated for severe cases refractory to conventional treatment6)
QCan I use oxerbelate while wearing contact lenses?
A
Contact lenses must be removed before instillation. They can be reinserted at least 15 minutes after instillation. For concomitant use with therapeutic contact lenses, follow the attending physician’s judgment.
QCan it recur after treatment?
A
Cases of epithelial defect recurrence after cessation of senegermin administration have been reported. Particularly in NK associated with herpetic keratitis, recurrence due to viral reactivation may occur 2). Regular follow-up after treatment is important.
6. Pathophysiology and Detailed Mechanism of Action
The cornea is the most densely innervated tissue in the human body, with sensory nerves 300 to 400 times more abundant than in the skin. Sensory nerves originating from the first branch of the trigeminal nerve (ophthalmic nerve) govern corneal sensation.
Corneal nerves maintain corneal epithelial homeostasis through neurotransmitters such as substance P, calcitonin gene-related peptide (CGRP), neuropeptide Y (NPY), and vasoactive intestinal peptide (VIP). Loss of these neural factors predisposes the corneal epithelium to damage, and once a wound forms, healing is delayed.
NGF binds to two types of receptors to exert its effects4).
TrkA (high-affinity receptor): The main receptor that promotes neuronal differentiation and survival. It is also involved in corneal epithelial cell proliferation, migration, and differentiation.
p75NTR (low-affinity receptor): Modulates NGF signaling together with TrkA. It is also involved in the regulation of apoptosis.
Mature NGF exerts its activity as a β-NGF dimer (molecular weight 26 kDa) 4).
Cenegermin (rhNGF) exerts the following pleiotropic effects.
Corneal epithelial repair: Promotes proliferation, migration, and adhesion of corneal epithelial cells, accelerating healing of epithelial defects.
Recovery of corneal sensation: Promotes regeneration of corneal sensory nerves, leading to improvement in corneal sensation2)3)
Promotion of tear production: Activates receptors in the lacrimal gland to stimulate tear secretion
Maintenance of limbal stem cell potential: Maintains the function of corneal epithelial stem cells
Anti-inflammatory effect: Suppresses TLR3-induced NF-κB activation and reduces excessive production of reactive oxygen species1). Also contributes to improved graft survival after corneal transplantation
Zambino et al. (2021) proposed two mechanisms for the resolution of hypopyon by cenegermin: resolution of inflammation accompanying epithelial defect closure and the immunomodulatory effect of NGF itself (suppression of inflammatory cytokines such as IFN-γ and TNF-α)1).
7. Latest Research and Future Perspectives (Research Stage Reports)
García-Delpech et al. (2022) administered cenegermin to 5 patients with Stage II-III NK, and confirmed ulcer healing and improvement in corneal sensation in all cases. During a 4-year long-term follow-up, no recurrence of corneal ulcer was observed in any case3).
Bu et al. (2022) reported treatment outcomes in 4 cases (3 adults and 1 child aged 9 years). All cases achieved epithelial closure and improvement in corneal sensation, and corneal stability was maintained during a follow-up of up to 32 months. However, viral reactivation was observed in 2 patients with herpetic keratitis2). Off-label use in a 9-year-old girl remained stable for 31 months, suggesting efficacy in children2).
DEFENDO trial: An 8-week open-label prospective study targeting Stage 1 NK. 37 patients were enrolled, and long-term follow-up for 24–30 months is ongoing.
PROTEGO trial: A phase III study targeting severe dry eye associated with Sjögren’s syndrome. Senegermin 20 μg/mL is administered 3 times daily for 4 weeks. Expansion of indication from NK to dry eye is being investigated5).
IRIS registry study: The efficacy of NGF treatment was confirmed from large-scale real-world data of 31,316 cases.
Cost-effectiveness: In Germany, it costs about 20,000 euros for 8 weeks, which is expensive, and in 2020, the G-BA (Federal Joint Committee) withdrew it from the German market 2). Cost reduction is key to widespread adoption.
Low-dose, long-term regimen: For cases without epithelial defects such as NK after LASIK, long-term administration at low concentration and low frequency is being investigated.
Comparison with corneal nerve regeneration surgery: Determining the optimal use of cenegermin and corneal nerve regeneration surgery for severe NK is a future challenge 6).
Zambino N, Syed ZA. Resolution of a neurotrophic keratopathy associated hypopyon with cenegermin. American journal of ophthalmology case reports. 2021;23:101113. doi:10.1016/j.ajoc.2021.101113. PMID:34307960; PMCID:PMC8296075.
Bu JB, Gericke A, Pfeiffer N, Wasielica-Poslednik J. Neurotrophic keratopathy: Clinical presentation and effects of cenegermin. American journal of ophthalmology case reports. 2022;26:101488. doi:10.1016/j.ajoc.2022.101488. PMID:35330588; PMCID:PMC8938625.
García-Delpech S, Udaondo P, Fernández-Santodomingo AS, García-Teillard D. Neurotrophic Keratopathy Treated with Topical Recombinant Human Nerve Growth Factor (Cenegermin): Case Series Study with Long-Term Follow-Up. Case reports in ophthalmology. 2022;13(2):663-670. doi:10.1159/000525923. PMID:36160492; PMCID:PMC9459538.
Kanu LN, Ciolino JB. Nerve growth factor as an ocular therapy: applications, challenges, and future directions. Semin Ophthalmol. 2021;36(4):224-231.
Pflugfelder SC, Massaro-Giordano M, Perez VL, et al. Topical recombinant human nerve growth factor (cenegermin) for neurotrophic keratopathy: a multicenter randomized vehicle-controlled pivotal trial. Ophthalmology. 2020;127(1):14-26. (TFOS DEWS III Management and Therapy Reportより引用)
Pham CM, Tran KD, Lee EI, et al. Corneal neurotization for the treatment of neurotrophic keratopathy: current perspectives. Curr Opin Ophthalmol. 2025;36(4):294-301.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.