Perforating injury
Definition: Both entry and exit wounds are present.
Also called double perforation, with ocular contents protruding from two sites (front and back). Severity is relatively high.

A perforating eye injury, based on the Birmingham Eye Trauma Terminology, is defined as a laceration caused by a sharp object with both an entry and an exit wound. It is an open globe injury that penetrates the eye wall from front to back, resulting in both an entry and an exit wound.
It is clearly distinguished from penetrating eye injury (entry wound only) and globe rupture (caused by blunt force). Perforating injury is also called double perforation and is more severe than penetrating injury because it involves two wounds (front and back).
Perforating injury
Definition: Both entry and exit wounds are present.
Also called double perforation, with ocular contents protruding from two sites (front and back). Severity is relatively high.
Penetrating injury
Definition: Only an entry wound is present.
There is no exit wound, and no penetration into the posterior segment. Relatively milder than perforating injury.
Globe rupture
Definition: A condition in which the cornea or sclera is separated due to a sudden increase in intraocular pressure caused by blunt force.
It is caused by blunt trauma rather than a sharp object.
The injury site affects prognosis and is classified into the following three zones1). In perforating injuries, the exit wound often reaches Zone III, posing a high risk of posterior segment damage.
| Zone | Extent | Characteristics |
|---|---|---|
| I | Cornea to limbus | Limited to anterior segment |
| II | Up to 5 mm posterior to the limbus | Anterior to the ora serrata |
| III | More than 5 mm posterior to the limbus | Posterior segment including the retina |
| Item | Penetrating | Perforating |
|---|---|---|
| Number of wounds | Entry wound only | Entry + exit wounds |
| Severity | Relatively mild | Relatively severe |
| Ocular content prolapse | Only at entry site | Two sites (anterior and posterior) |
| Posterior segment injury | Less common | Frequent (Zone III) |
| Vitrectomy frequency | Low | High |
The incidence of ocular trauma is estimated at approximately 3.5–4.5 per 100,000 people 1). The majority of patients are male, with a relative risk about 5.5 times higher than females, and the average age at injury is around 30 years.
In children, the incidence of severe ocular trauma is 11.8 per 100,000 per year. Children account for over 35% of severe ocular trauma, and most are under 12 years old. Because of the added risk of amblyopia, prompt management is especially important in children.
A perforating ocular injury has both an entry and an exit wound (double perforation), whereas a penetrating injury has only an entry wound without an exit wound. In perforating injuries, ocular contents may prolapse from both anterior and posterior sites, and posterior segment damage (Zone III) is common, making it more severe than penetrating injuries. The frequency of requiring vitrectomy is also higher in perforating injuries.
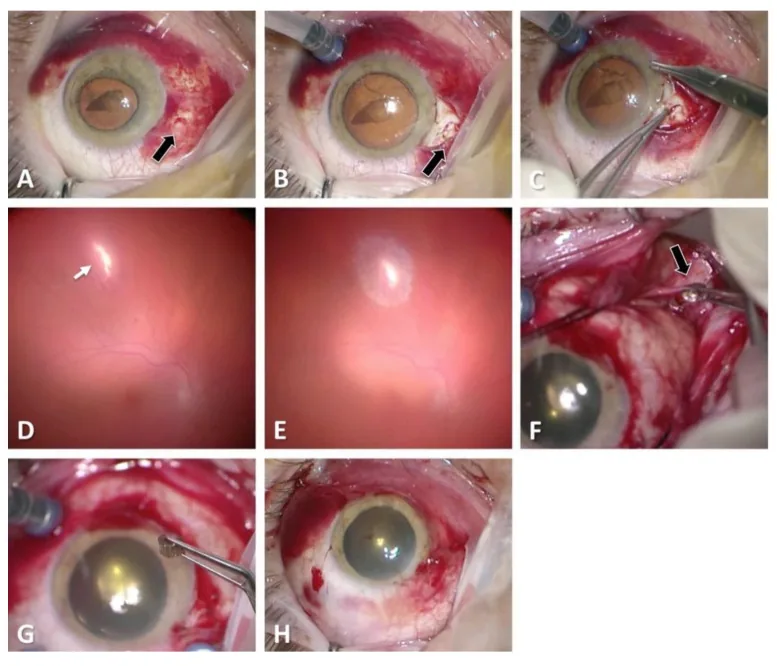
The following findings are characteristic of perforating injury:
The Seidel test using fluorescein staining is useful for evaluating full-thickness wounds. Under cobalt blue light, the dye is washed away by aqueous humor leakage (Seidel positive), confirming a full-thickness wound.
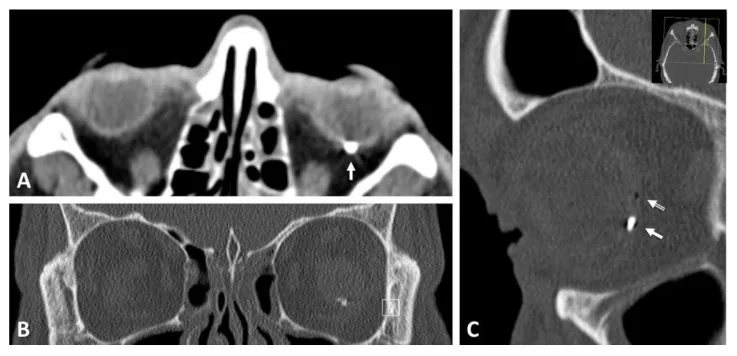
If there is low intraocular pressure, severe subconjunctival hemorrhage, or hyphema, open globe injury should be suspected. Even if anterior segment findings are mild, if there is a history of injury from a high-speed projectile or stab wound, consider the possibility of perforation and perform CT imaging. If there is an entry wound, CT (1 mm slices) is essential to check for an exit wound in the posterior segment.
Perforating ocular injuries occur when a sharp object penetrates the eyeball with sufficient force.
Blast injuries can result in multiple perforating wounds. In the Beirut port explosion (2020), 39 patients with 48 eyes were injured, with open globe injuries in 10 eyes (20.8%) 2). Although 54.2% were superficial injuries, 53.8% required surgical intervention. Fragments and flying glass from the explosion were the main causes of injury 2).
The incidence of endophthalmitis in open globe injuries is 2–7%. Infections originating from plants or soil lead to blindness at a high rate. Unlike postoperative endophthalmitis after cataract surgery, endophthalmitis caused by virulent bacteria such as Bacillus species is a concern. In orbital foreign bodies, anaerobic infections (e.g., tetanus) should also be considered.
In explosions, both the blast wave itself and flying metal or glass fragments damage the eye. In a survey after the Beirut port explosion, 10 out of 48 eyes (20.8%) in 39 patients sustained open globe injuries, mainly caused by flying glass and debris 2). Blast trauma differs from ordinary eye trauma in that it often results in multiple perforations and bilateral eye injuries.
The diagnosis of open globe injury is made through a combination of detailed history taking, careful examination, and imaging studies.
Obtain detailed information on the time, mechanism, and causative object of the injury. Also check for protective eyewear use, tetanus immunization status, and time of last meal (due to possible general anesthesia). In patients with decreased consciousness, it is important to gather information from family members or others involved.
| Imaging modality | Main indications | Notes |
|---|---|---|
| Orbital CT | Foreign body detection, globe deformation, location of exit wound | 1 mm thin slices recommended; indicated in all cases |
| B-mode ultrasound | Evaluation of posterior segment when media opacity | Avoid pressure. Use caution if open wound suspected |
| X-ray | Detection of metallic foreign bodies | Detectable if ≥2mm and thickness ≥0.4mm |
CT scan is indicated for all cases of penetrating ocular trauma. It can simultaneously evaluate the location of intraocular foreign bodies, globe deformation, orbital fractures, and intracranial lesions, and can confirm the extension of the exit wound to the posterior segment. Thin-slice (1mm) sections are recommended.
Additional confirmation in penetrating trauma: If the exit wound is in the posterior segment (Zone III), confirm its location on both axial and sagittal CT views. The closer to the posterior pole, the greater the impact on visual function.
MRI is contraindicated if a metallic foreign body is suspected. It can only be used to confirm non-metallic foreign bodies (e.g., wood fragments, deep fluid collections).
The priority in treating penetrating ocular trauma is wound closure (primary repair) to prevent infection and extrusion of ocular contents.
Primary repair within 24 hours of injury is recommended. A systematic review and meta-analysis (15 studies, 8,497 eyes) showed that repair within 24 hours reduces the risk of endophthalmitis with an odds ratio of 0.39 (95% CI 0.19–0.79)1). General anesthesia is typically selected.
Use 10-0 nylon. Aim for watertight closure, but avoid overtightening sutures as it can cause corneal astigmatism and irregular astigmatism; take longer bites.
Use 7-0 nylon as the basic suture, selecting 6-0 to 8-0 nylon depending on the wound location. First, secure the four rectus muscles and explore the wound. If the wound is deep and the rectus muscle obstructs, temporarily detach the tendon. For limbal wounds, first suture with 9-0 nylon, then close the corneal wound with 10-0 nylon and the scleral wound with 9-0 nylon using interrupted sutures.
If the exit wound is in the posterior segment (Zone III), detachment and rotation of the extraocular muscle may be necessary. Explore and suture the posterior scleral wound under direct visualization. Wounds near the posterior pole are technically difficult to suture and should be handled by an experienced surgeon.
Administer systemic broad-spectrum antibiotics covering gram-positive and gram-negative bacteria. Combination therapy with vancomycin and a third-generation cephalosporin (e.g., ceftazidime) is associated with a reduced incidence of endophthalmitis.
If endophthalmitis is suspected, early surgical intervention is recommended. If inflammation is confined to the anterior chamber, perform anterior chamber washout and inject vancomycin 1 mg/0.1 mL and ceftazidime 2.25 mg/0.1 mL into the anterior chamber and vitreous cavity. If vitreous opacification is extensive, perform emergency vitrectomy.
In perforating injuries, posterior segment damage is frequent, so the proportion requiring secondary surgery (vitrectomy) is higher than in penetrating injuries. In the following cases, consider performing vitrectomy immediately after primary repair.
Three-port vitrectomy is performed to remove the opaque vitreous and release incarcerated vitreous. Gas tamponade or silicone oil tamponade is used to achieve retinal reattachment and ensure visibility.
Primary repair within 24 hours of injury is strongly recommended. Systematic reviews and meta-analyses have shown that repair within 24 hours reduces the risk of endophthalmitis with an OR of 0.39 (95% CI 0.19–0.79) 1). However, within 24 hours, no significant difference in final visual acuity was found between earlier and later repair timing (OR 0.89, 95% CI 0.61–1.29) 1). Comparison of even earlier time windows within 24 hours remains a topic for future research.
A sharp object penetrates the anterior surface of the eyeball (cornea or anterior sclera) and exits through the posterior surface (posterior sclera). During this process, intraocular contents (vitreous, uvea) prolapse through both the entry and exit wounds, leading to ocular collapse. Unlike penetrating trauma, perforating injury is characterized by prolapse and damage of intraocular contents at the exit wound as well.
When the exit wound reaches Zone III (5 mm or more posterior to the limbus), direct damage to the retina, choroid, and optic nerve occurs. Vitreous gel may become incarcerated in the wound, and contraction can cause traction that tears the opposite retina.
In perforating injuries, there are two sites of vitreous incarceration (entry and exit), so traction occurs from multiple directions, often leading to complex retinal detachment.
The following secondary changes may occur after initial treatment of the injury:
McMaster et al. (2025) conducted a systematic review and meta-analysis on the timing of primary repair after open globe injury and its association with visual outcomes and endophthalmitis rates 1). Analyzing 15 studies involving 8,497 eyes, they reported the following results.
The authors strongly recommend repair within 24 hours, but more detailed timing comparisons, such as emergency nighttime surgery versus next-morning surgery, await future prospective studies 1).
Kheir et al. (2021) reported a case series of 39 patients (48 eyes) who sustained ocular trauma after the Beirut port explosion in August 2020 2). Key findings are as follows.
For blast injuries, it is important to prepare systems for multiple wounds and injuries to multiple eyes.
The Ocular Trauma Score (OTS) is a prognostic tool that estimates the probability of visual outcomes based on initial visual acuity, presence of globe rupture, endophthalmitis, penetrating injury, retinal detachment, and relative afferent pupillary defect (RAPD). In a study of 93 combat-related ocular trauma cases, the sensitivity for predicting visual survival (light perception or better) was 94.8%, and the specificity for predicting no light perception was 100%. The OTS is useful for determining treatment strategies and counseling patients with penetrating injuries.