Cyclodialysis cleft refers to a condition in which the longitudinal fibers of the ciliary muscle separate from the scleral spur, forming a direct communication between the anterior chamber and the suprachoroidal space. Through this communication, aqueous humor excessively drains into the suprachoroidal space, leading to ocular hypotony.
Many clefts close spontaneously, but if they do not, chronic hypotony may develop. Persistent hypotony can cause hypotony maculopathy, optic disc edema, and visual loss.
The most common cause is blunt trauma, but it can also occur after intraocular surgeries such as trabeculectomy, goniotomy, cataract surgery, and MIGS (micro-invasive glaucoma surgery) 1). Even after blunt trauma, the incidence is low and easily overlooked.
In the past, intentional creation of a cyclodialysis cleft was used as a treatment for open-angle glaucoma, but this is rarely performed today.
QWhat is a cyclodialysis cleft?
A
Cyclodialysis is a condition in which the ciliary body detaches from the scleral spur (the skeletal structure of the angle), creating a direct communication between the anterior chamber and the suprachoroidal space. This causes aqueous humor to flow excessively into the suprachoroidal space instead of the normal outflow pathway, leading to a marked decrease in intraocular pressure. The main causes are severe blunt trauma to the eye or intraocular surgery. In many cases, it closes spontaneously, but if it does not close, treatment is necessary to prevent visual impairment due to hypotony.
By definition, increased aqueous outflow through the dialysis leads to suprachoroidal fluid, but visible choroidal detachment or shallowing of the anterior chamber is not a common finding. A remote history of ocular trauma is also important, as a previously closed dialysis may reopen during surgery.
The causes of cyclodialysis are broadly divided into traumatic and iatrogenic.
Blunt trauma: The most common cause. A sudden increase in anterior chamber pressure causes the ciliary muscle to detach from the scleral spur. Often accompanied by hyphema and angle recession.
Trabeculectomy: Can occur after glaucoma surgery. Mechanism differs from postoperative overfiltration.
Goniotomy/Trabeculotomy: As a complication of pediatric glaucoma surgery.
Cataract surgery: Due to manipulation during phacoemulsification.
MIGS: A case has been reported of a 65-year-old woman who developed cyclodialysis during MIGS, with persistent hypotony for 11 months3).
In trauma, a tear occurs between the longitudinal and circular fibers of the ciliary muscle, and the ciliary body moves posteriorly together with the iris. The injury site shifts stepwise toward the sclera: iris root (iridodialysis), within the ciliary body (angle recession), and between ciliary body and sclera (cyclodialysis).
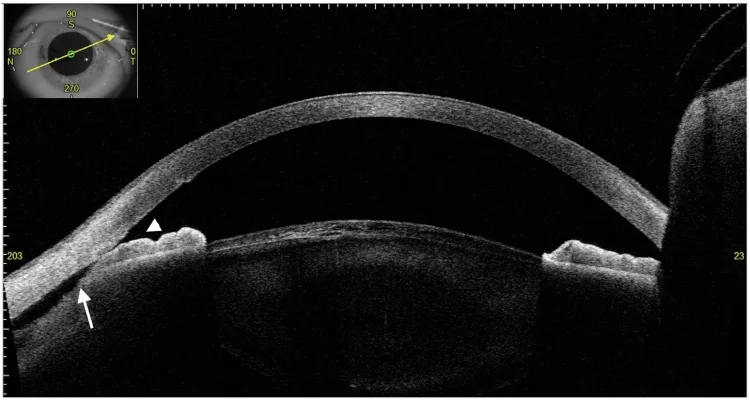
Cureus. 2025;17(1):e77516. Figure 4. PMCID: PMC11743908. License: CC BY.
Anterior segment OCT shows a cleft associated with ciliary body detachment. The separation between the scleral spur and ciliary body can be seen in cross-section.
On gonioscopy, cyclodialysis is observed as an abnormally deep area posterior to the scleral spur. The iris root and ciliary body are displaced posteriorly. The cleft appears white (scleral-like), black, or gray.
However, evaluation of the angle is difficult in eyes with shallow or flat anterior chamber due to hypotony, or in the presence of corneal edema or hyphema. Injection of viscoelastic material into the anterior chamber may improve visibility. The cleft may be hidden adjacent to extensive peripheral anterior synechiae, requiring careful search.
Ultrasound biomicroscopy uses a high-frequency B-mode transducer (50–100 MHz) to image anterior segment structures with high resolution of 25–50 μm. It is the best method for identifying the presence, size, and associated suprachoroidal fluid of cyclodialysis.
Clefts not detectable by gonioscopy can be identified by ultrasound biomicroscopy, which is useful as an adjunctive diagnosis when cyclodialysis is suspected in post-traumatic hypotony 1). It can also be used in the presence of corneal opacity.
AS-OCT has the advantage of being non-contact and rapid, but pigmentation on the posterior surface of the iris hinders light transmission, making adequate visualization of the ciliary body and suprachoroidal space difficult. Corneal opacity also degrades image quality. Its utility in evaluating cyclodialysis is limited.
Ultrasound biomicroscopy (UBM) is the most excellent examination method. Small detachments that cannot be detected by gonioscopy can be identified by UBM, and it can be used even in the presence of corneal opacity. Anterior segment OCT is non-contact and simple, but its usefulness is limited because iris pigment restricts visualization of the ciliary body.
Cycloplegics are first-line treatment. By relaxing the ciliary muscle and expanding the ciliary ring, the detached muscle fibers are brought into close contact with the sclera.
1% atropine sulfate eye drops: 1–2 times daily, used for up to 6–8 weeks
Steroid eye drops: Opinions are divided between using them for anti-inflammatory purposes and deliberately reducing them to promote ciliary-scleral adhesion.
If cyclodialysis does not improve within 1–2 weeks, proceed to the next step. Many cases improve with conservative treatment alone. However, if intraocular pressure is 4 mmHg or lower, it is necessary to restore pressure within 2 months.
Indicated when pharmacotherapy fails to close the detachment. It induces local inflammation, promoting adhesion between the choroid and sclera to seal the detachment.
Argon laser: Applied to the sclera, ciliary body, and iris at the detachment site. Settings: power 0.3–3 W, spot size 200 μm, duration 0.5 seconds
Transscleral diode laser: Using a G-probe. Power 1500–2500 mW, duration 1500–2000 ms
Endolaser: Coagulation of both walls of the dissection using an 810 nm diode laser endoscope. Considered for children and small dissections.
Coagulation is performed with a green or yellow wavelength laser to cause slight contraction of the ciliary body and deposition of a small amount of fibrin.
Cryotherapy: Indicated for relatively small detachments within 3 hours. Perform 2-3 freeze-thaw cycles at -85°C. Initial success rate 36-50%.
Diathermy: Apply diathermy pins under a partial-thickness scleral flap. Treatment area should not exceed 4 hours.
Internal Approach
Direct cyclopexy: The most well-studied method. Under a scleral flap, directly visualize the ciliary body and suture it to the sclera with 8-0 to 9-0 nylon. Initial success rate 67-96%, nearly 100% after a second procedure.
Transanterior cyclopexy: Indicated for pseudophakic and aphakic eyes. No scleral flap required; simpler technique.
Other reported methods include SF6 gas injection, gas injection combined with vitrectomy, temporary scleral buckling, placement of IOL haptics in the ciliary sulcus, and suturing of a capsular tension ring (CTR).
Intraocular pressure (IOP) elevation may occur after closure of the detachment, usually transient. It can often be managed with topical IOP-lowering medications, oral carbonic anhydrase inhibitors, and hyperosmotic agents, but rarely requires filtering surgery 1,2).
A case has been reported in which two consecutive cyclodialysis clefts occurring after MIGS were sequentially closed, resulting in two equal IOP spikes of 55 mmHg and 54 mmHg 3). This is difficult to explain by conventional compensatory mechanisms (increased aqueous production or decreased trabecular outflow), as the second spike would be expected to be smaller after partial normalization following the first closure. This suggests a direct response to the closure itself 3).
QWhy does intraocular pressure increase after closure of a cyclodialysis cleft?
A
The exact mechanism is unknown, but two main hypotheses exist: (1) Compensatory increased aqueous production by the ciliary body to counter excessive outflow through the cleft persists temporarily after closure; (2) The trabecular meshwork and Schlemm’s canal outflow function decreases (collapse, fibrosis) while the cleft is open and takes time to normalize. A recent case report also suggests a direct response to the closure itself.
The ciliary muscle consists of three layers: longitudinal (Brücke’s muscle), oblique, and circular (Müller’s muscle), all of which attach anteriorly to the scleral spur. In blunt trauma, a sudden rise in intraocular pressure causes the limbus to stretch, and aqueous humor moves posteriorly and into the angle, placing mechanical stress on the iris and ciliary body.
Injury ranges from mild to severe, progressing sequentially from rupture of the iris root (iridodialysis) to cleft formation within the ciliary body (angle recession) to complete detachment of the ciliary body from the sclera (cyclodialysis).
When cyclodialysis creates a direct communication between the anterior chamber and the suprachoroidal space, aqueous humor flows in large amounts into the suprachoroidal space without passing through the normal uveoscleral outflow pathway. In addition, reduced aqueous production by the damaged ciliary body may also contribute.
Marked hypotony causes the posterior segment to collapse anteriorly, leading to the formation of folds in the macula. It can occur at intraocular pressures below 10 mmHg, but the incidence increases below 5 mmHg. If pressure remains below 4 mmHg for 2–3 months, visual recovery is poor, and metamorphopsia and relative central scotoma tend to persist. Young patients and those with high myopia are risk factors.
Mechanism of intraocular pressure spike after closure
Multiple mechanisms are hypothesized for the rise in intraocular pressure after closure of the cyclodialysis cleft1,2).
Compensatory increase in aqueous production: Aqueous production by the ciliary body increases to counteract excessive outflow through the cleft, and this increase may persist temporarily even after closure.
Reduced trabecular outflow: While the cleft is open, the trabecular meshwork and Schlemm’s canal may collapse or become fibrotic, reducing outflow function.
Direct response to cleft closure itself: In a case where two cyclodialysis clefts after MIGS closed sequentially and produced equivalent intraocular pressure spikes (55/54 mmHg), the compensatory mechanism alone cannot explain the second equivalent spike, suggesting that closure itself may trigger a pressure rise through some mechanism3).
A case report of two cyclodialysis clefts after MIGS that closed sequentially, each producing an equivalent intraocular pressure spike (55/54 mmHg), presents a phenomenon that cannot be fully explained by the conventional compensatory increase hypothesis3). It suggests that cleft closure itself may directly induce a rise in intraocular pressure, and elucidating this mechanism is an important future task3).
Generally, intervention within 3 months is recommended, but cases of visual recovery after months to years of hypotony have also been reported. Even in long-standing cyclodialysis, treatment should not be hesitated. If intraocular pressure remains at 4 mmHg or lower, recovery of intraocular pressure within 2 months is desirable.
Since eyes with resolved cyclodialysis involve at least some degree of angle recession, long-term follow-up is necessary to monitor for the future development of angle recessionglaucoma.
Ioannidis AS, Barton K. Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmol. 2010;21(2):150-4. PMID: 20051856.
Ioannidis AS, Bunce C, Barton K. The evaluation and surgical management of cyclodialysis clefts that have failed to respond to conservative management. Br J Ophthalmol. 2014;98(4):544-9. PMID: 24457370.
Alshaikhsalama A, Nathan N. Cyclodialysis clefts following microinvasive glaucoma surgery with consecutive intraocular pressure spikes. Case Rep Ophthalmol Med. 2022;2022:7595507. PMID: 36312842.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.